Pricing strategies for pharmaceuticals in developing countries: what options do we have?
|
Abstract:
Effective pharmaceutical pricing policies in developing countries are important to ensure accessibility and affordability of essential medicines for the people.
|
Submitted: 24 October 2016; Revised: 27 February 2017; Accepted: 28 February 2017; Published online first: 13 March 2017
In developing countries, essential medicines are not always available to those who need them because of prohibitive prices and lack of availability, and the quality of medicines and healthcare are also variable [1]. About one-third of the world’s population lack sustainable access to essential medication [2]. This is most pronounced in poor countries. Despite the existence of pharmaceutical pricing policies in some of these countries, the evidence does not always support their effectiveness in improving prices and availability.
Governments have a responsibility to ensure that all citizens receive affordable health care and medicines, and can do this by controlling different stages of the pharmaceutical supply chain. The World Health Organization (WHO) has produced guidelines for low- and middle-income countries on how to implement effective pharmaceutical pricing policies [3]. These include regulation of mark-ups in the pharmaceutical supply and distribution chain; tax exemptions/reductions for pharmaceutical products; application of cost-plus pricing formulae for pharmaceutical price setting; use of external reference pricing; promotion of use of generic medicines; and use of health technology assessment.
In developing countries, including the Middle East and North Africa, the pharmaceutical sector is relatively unregulated, and the extent of regulation depends on level of income, policies and degree of inclusion of the healthcare system in the national vision. This can occasionally affect the availability and affordability of certain drugs. Temporary deficits in the procurement of affordable essential medicines can negatively affect patients with non-communicable diseases, notably the pharmaceutical management of chronic cardiovascular diseases highly prevalent in Middle Eastern and North African countries [4].
We conducted a literature review to evaluate whether the inefficiency of the pharmaceutical sector is a result of absence of policies or lack of implementation and enforcement of policies in developing countries. The review covered English and Arabic scientific journals (including both experimental and observational studies) and government publications published between January 2000 and March 2016 covering pharmaceutical pricing policies and their effect. The search was conducted across several databases, including PubMed, PQ Central, EconLit, ProQuest, CINAHL, Scopus, ScienceDirect, Cochrane, WHOLIS, WHOCC, and Web of Knowledge. The search terms used were ‘drug’, ‘medicine’, ‘pharmaceutical’, ‘price, pricing’, ‘price containment’, ‘price control’, ‘pricing strategy’, ‘pricing policy’, and ‘developing countries’ or ‘LMICs’ where applicable. Grey literature search was also conducted through government publications, WHO/HAI reports and Open Grey database in addition to using the search engine Google Scholar. This search yielded 1,250 studies. After removing duplicates and screening against the inclusion criteria, i.e. descriptive or quasi-experimental policies, initiatives and strategies to control prices, 87 publications were identified for full-text screening. This produced 25 eligible studies which were included in the systematic review, see Table 1. Eighteen covered Asian countries, five from African countries, two from South America, and one from Mexico.
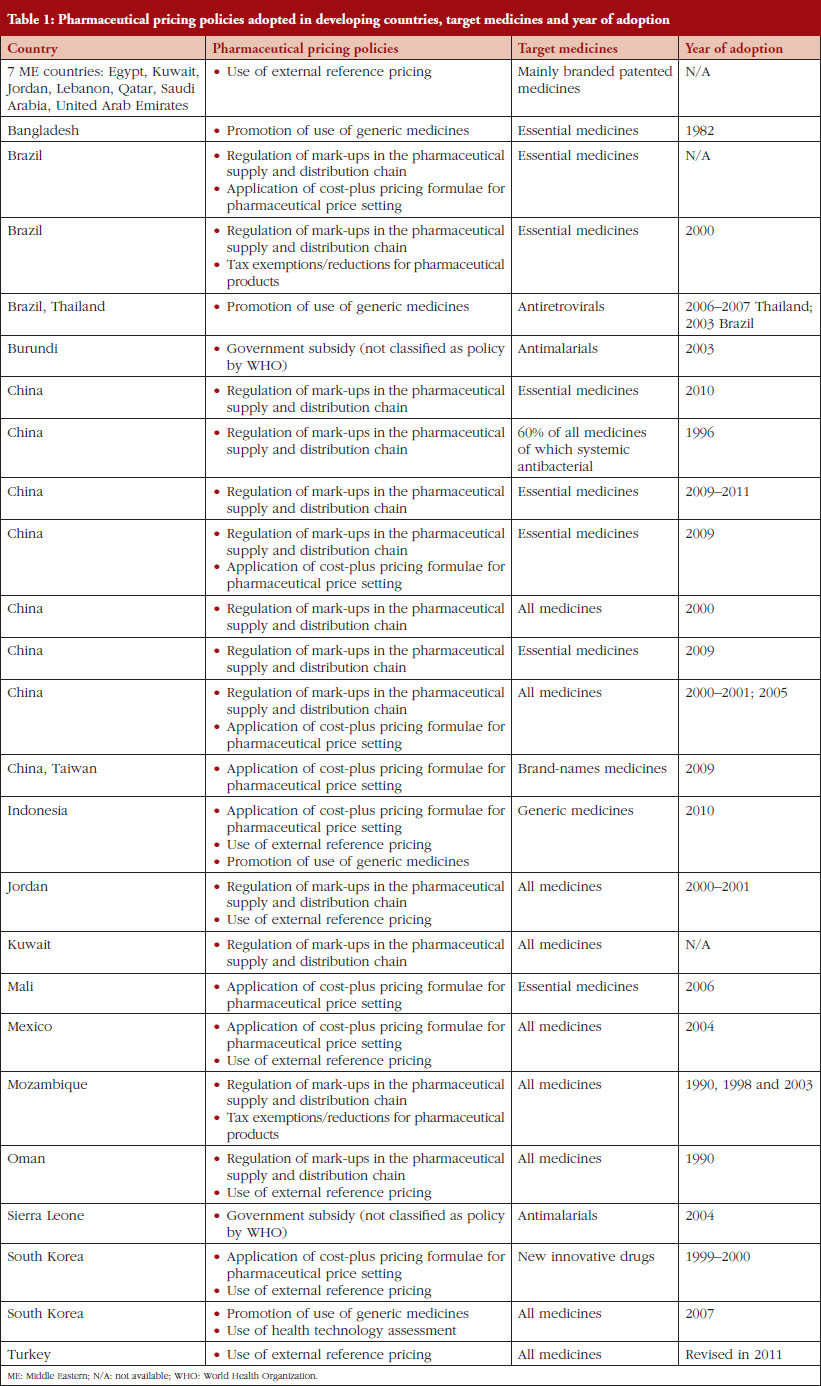
The policies identified in the eligible studies pertained mainly to disease-specific and essential medicines, see Table 1. These policies were mapped to the WHO guidelines on pharmaceutical pricing policies [3]. An explorative synthesis of the 25 included studies showed that the most commonly used policies are external reference pricing and mark-up regulation, whereas tax exemptions and health technology assessment were the least used. In most of the cases reviewed, policies have been ineffective because of poor legislative framework, lack of pre- and post-implementation activities, and non-compliance by various stakeholders. Six out of the 25 studies were quasi-experimental (pre-/post-implementation), which allowed for a qualitative synthesis. Due to the diversity of outcomes measured, a quantitative comparison was not possible; nevertheless, the policies demonstrated a favourable impact toward lowering the price of medicines. These decreases in prices were undermined by either an increase in utilization, or long periods for the decreases to occur.
The volume of publications available was surprisingly low, and in many cases, the quality of reporting was poor. In these studies, the pricing strategies were mentioned but no outcome was identified.
Due to the unique nature of medicine, the commercial aspects related to pharmaceuticals should consider the therapeutic, psychological and human value they add to society. These aspects include procurement, availability, affordability and quality. Therefore, governments and stakeholders should collaborate and commit to tailor a pharmaceutical pricing policy that respects the uniqueness of an individual market and its economics capacity. The study designs identified in the included studies reflected the weak monitoring activities undertaken by policymakers or governments to evaluate the impact of the policies implemented. Such evaluative studies can provide decision-makers with evidence-based measurement of the effectiveness of price containment strategies adopted. No relationship was identified between the economic status of a country and the type of pricing policy implemented. The promotion of generic medicines use was remarkably low in developing countries despite the tremendous benefits that would be brought to societies. Generics use can lessen the economic burden on consumers and payers; however, its low rate of prescription is correlated to social beliefs and attitudes of both prescribers and consumers, to low profit margins, and to lack of pro-generics regulation.
Although many developing countries have implemented pricing strategies, it is vital that more research is conducted to ascertain the shortcomings of such policies, ultimately leading to the required reforms.
Competing interests: None.
Provenance and peer review: Not commissioned; externally peer reviewed.
Co-author
Nada Moustafa Abdel Rida, MSc Candidate
College of Pharmacy, Qatar University, PO Box 2713, Doha, Qatar
References
1. Niens LM, Cameron A, Van de Poel E, Ewen M, Brouwer WB, Laing R. Quantifying the impoverishing effects of purchasing medicines: a cross-country comparison of the affordability of medicines in the developing world. PLoS Med. 2010;7(8). pii: e1000333. doi.org/10.1371/journal.pmed.1000333
2. World Health Organization and Health Action International. Measuring medicines prices, availability, affordability and price components. 2nd ed. Geneva: World Health Organization; 2008.
3. Cameron A, Hill S, Whyte P, Ramsey S, Hedman L. WHO guideline on country pharmaceutical pricing policies. Geneva: World Health Organization; 2015.
4. Almahmeed W, Arnaout MS, Chettaoui R, Ibrahim M, Kurdi MI, Taher MA, et al. Coronary artery disease in Africa and the Middle East. Ther Clin Risk Manag. 2012;8:65-72.
|
Author for correspondence: Professor Mohamed Izham Mohamed Ibrahim, PhD, Professor of Social & Administrative Pharmacy, College of Pharmacy, Qatar University, PO Box 2713, Doha, Qatar
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2017 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/pricing-strategies-for-pharmaceuticals-in-developing-countries-what-options-do-we-have.html
Generic medicines entry into the Malaysian pharmaceutical market
Author byline as per print journal: Omotayo Fatokun, PhD; Professor Mohamed Izham Mohamed Ibrahim, PhD; Professor Mohamed Azmi Hassali, PhD
|
Abstract:
There are major barriers to generic medicine development and market entry in Malaysia. This mixed method study recommends strategies to increase uptake.
|
Submitted: 25 October 2016; Revised: 15 November 2016; Accepted: 21 November 2016; Published online first: 28 November 2016
Due to the rising costs of pharmaceuticals and a prevailing economic crisis, the availability of generic equivalents of trademark innovator medicines has become crucial to the Malaysian healthcare system. In 2003, Malaysia became the first country in Asia to issue a compulsory licence for the importation of generic versions of patented antiretroviral medicines, following the adoption of the World Trade Organization (WTO) Doha declaration on the Trade-Related Aspects of Intellectual Property Rights (TRIPS) agreement and public health. [1, 2]. This action was taken to increase access to affordable antiretroviral medicines, patented forms of which were highly priced. As a result of the licence, the average treatment costs per HIV-infected patient per month in public hospitals declined by up to 83% and there were widespread reductions in the prices of innovator patented antiretroviral products [1, 3]. Nevertheless, issues surrounding pharmaceutical patents mean medicine accessibility and generics availability continue to be a challenge in Malaysia [2].
The summary of the findings from a study on generic medicines entry into the Malaysian pharmaceutical market is presented in this paper. The determinants and characteristics of generic medicines entry following the patent expiration of innovator drug products in Malaysia were investigated. The sources of data used for the work included 22 policy documents, a survey of 13 key informants, a cross-sectional questionnaire of 14 generic medicines manufacturing industries, and panel data analysis of the 12 best-selling single entity prescription drug products that experienced loss of patent protection and subsequent generics entry in Malaysia between January 2001 and December 2009 [4].
The study began with analysis of policy documents, followed by semi-structured interview and qualitative questionnaire survey. The policy analysis included analysis of policy content, outputs and processes. The documents were restricted to publicly available and nationally-applicable official documents from government sources (print or Internet-based). These documents include laws, regulations, rules, policies, administrative orders, directives, guidelines, reports and other documented statements issued by the government, ministries, departments and agencies that were intended to directly or indirectly affect the production, distribution, prescribing, dispensing and the use of medicines in Malaysia. The key informants’ survey consisted of semi-structured interviews and self-completed qualitative questionnaire. The potential key informants were selected using a purposive non-probabilistic sampling, i.e. on the basis of their key position, professional expertise and good knowledge of the generic medicines environment in Malaysia. The 13 key informants were from seven organizations, i.e. the Malaysian Organization of Pharmaceutical Industries, generic medicines importers, Malaysian Medical Association, Malaysian Pharmaceutical Society, Federation of Malaysia Consumers Associations, Malaysian Pharmaceutical Services Divisions, and National Pharmaceutical Control Bureau. Cross-sectional national surveys of a self-completed questionnaire were used among generic drug manufacturers. The final study design was the panel data analysis on ‘best-selling’ single entity prescription International Nonproprietary Name (INN) drug products that lost patent protection and experienced subsequent generics entry. The drugs selected in this study were based on the empirical justification that post-patent entry of generic medicines is driven by the sales value of the patented drug molecule before patent expiration. Initially, 64 INN drug products were selected and screened to determine their registration status. The registration status of the drug products were obtained from the list of approved products and the drug products registration database of the Malaysian National Pharmaceutical Control Bureau.
Fourteen categories of policies and regulatory measures with varying effects on generics entry in Malaysia were identified. The major factors driving generics development and market entry in Malaysia were the prepatent expiration market value of innovator products, the cost of generics development and approval, and compatibility with pharmaceutical firms’ existing product ranges. The innovator product’s prepatent expiration market value was also a significant entry driver, but more so for domestic generics firms than export-oriented companies.
The major barriers to generic medicine development and market entry identified were patent clustering by innovator firms and the earlier market entry of imported generics. Government policies and regulations were perceived by respondents to be fairly effective in promoting generic medicines in Malaysia. The majority of respondents were dissatisfied with generics prescribing and generic medicines understanding among healthcare professionals, but satisfied with generics dispensing.
For the 12 best-selling prescription drug products, a total of 154 generics entries occurred over the eight-year period under study. The highest proportion of the sample belong to the cardiovascular class of drugs, followed in equal proportions by respiratory and nervous system drug products, which reflects the burden of disease among the Malaysian population. The occurrence of market entry for these drugs is characterized by a sequential quadratic curvilinear trend. The time to entry of generics was significantly longer than the hypothesized time to entry of one day following the basic patent expiration of an innovator product. This hypothesis is based on the TRIPS-compliant regulatory exception provision (also known as the early working exception or Bolar provision), and is used to enable the development of generic medicines before innovator product patent expiration [5, 6]. Competition among 28 off-patent drugs, the majority of which had been on the market for several years, showed that increased generics availability reduces drug prices in the off-patent pharmaceutical market. These findings illustrate the importance of the unhindered entry of generic medicines following the patent expiration of innovator drug products.
In sum, the presence of a variety of government policies have had varying effects on the entry of generic medicines to the Malaysian pharmaceutical market. These policies are those related to intellectual property rights; medicines regulation and registration; pharmaceutical pricing and competition; and the demand-side policies measures on generics prescribing, dispensing and consumptions. Market entry was found to be determined by the prepatent sales value of innovator products, the cost of generics development, market entry competition and the existence of patent-related entry barriers. The pattern of generics entry was characterized by a sequential curvilinear trend, and the time to generics entry was found to be significantly delayed beyond the expiration of the equivalent innovator product’s basic patent.
To improve generic medicines entry into the Malaysian pharmaceutical market, it is recommended to: (i) increase coherence between intellectual property rights and health policies; (ii) improve the patent administration system and ensure strict adherence to the patentability criteria of novelty; (iii) discourage any linkage between drug marketing approval and patents, including requests for listing of patent information with the drug regulatory authority; (iv) make trade-related policy coherent with regard to market entry of imported generic medicines vis-a-vis locally produced generic medicines; (v) enhance domestic capacity in bioequivalence testing and manufacturing to ensure more cost-efficient production of generic medicines; (vi) implement policies relating to generic medicines consistently across both the public and private sectors of the Malaysian healthcare system; and (vii) increase education and awareness of generic medicines among healthcare professionals and the public to promote generics prescribing, dispensing and consumption [7, 8].
Competing interests: None.
Provenance and peer review: Not commissioned; internally peer reviewed.
Authors
Assistant Professor Omotayo Fatokun, PhD
Department of Clinical Pharmacy, Faculty of Pharmaceutical Sciences, UCSI University, No. 1 Jalan Menara Gading, Cheras, 56000 Kuala Lumpur, Malaysia
Professor Mohamed Izham Mohamed Ibrahim, PhD
Professor of Social and Administrative Pharmacy
College of Pharmacy, Qatar University, Al Tarfa, PO Box 2713, Doha, Qatar
Professor Mohamed Azmi Hassali, PhD
Discipline of Social and Administrative Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, 11800 Minden, Penang, Malaysia
References
1. Ling CY. Malaysia’s experience in increasing access to antiretroviral drugs: exercising the ‘government use’ option. Penang: Third World Network; 2006.
2. Smith RD, et al. Trade, TRIPS, and pharmaceuticals. Lancet. 2009;373(9664):684-91.
3. World Health Organization. Commission on Intellectual Property Rights, Innovation and Public Health (CIPIH). Musungu SF, Oh C. The use of flexibilities in TRIPS by developing countries: can they promote access to medicines? 2006 [homepage on the Internet]. [cited 2016 Nov 15]. Available from: http://www.who.int/intellectualproperty/studies/TRIPSFLEXI.pdf
4. Fatokun O. Assessment of policies, determinants and characteristics of generic medicines entry into the Malaysian pharmaceutical market [dissertation]. Universiti Sains Malaysia; 2014.
5. De Joncheere K, Rietveld AH, Huttin C. Experiences with generics. Int J Risk Saf Med. 2002;15(1):101-9.
6. European Commission. Pharmaceutical sector inquiry final report [homepage on the Internet]. [cited 2016 Nov 15]. Available from: http://ec.europa.eu/competition/sectors/pharmaceuticals/inquiry/staff_working_paper_part1.pdf
7. Kaplan WA, Wirtz VJ, Stephens P. The market dynamics of generic medicines in the private sector of 19 low and middle income countries between 2001 and 2011: a descriptive time series analysis. PLoS One. 2013;8(9):e74399.
8. Benjamin D, Swartz M, Forman L. The impact of evidence-based education on prescribing in a psychiatry residency. J Psychiatr Pract. 2011;17(2):110-7.
|
Author for correspondence: Professor Mohamed Izham Mohamed Ibrahim, PhD, Professor of Social and Administrative Pharmacy, College of Pharmacy, Qatar University, Al Tarfa, PO Box 2713, Doha, Qatar
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2016 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/generic-medicines-entry-into-the-malaysian-pharmaceutical-market.html
Generic medicines policy in Qatar
|
Abstract:
Qatar’s pharmaceutical market is likely to remain highly dependent on imports. The use of generic medicines remains a great challenge to the country.
|
Submitted: 18 December 2014; Revised: 28 January 2015; Accepted: 1 February 2015; Published online first: 13 February 2015
Qatar is the world’s richest country per capita. The country established its National Health Strategy 2011–2016 in line with the Qatar National Vision 2030, which aims to advance Qatar’s Healthcare Vision of creating a world-class, patient-centred healthcare system [1, 2]. There has been a huge increase in public spending on health care in Qatar, giving it the highest per capita health expenditure in the Middle East. The National Health Insurance Scheme is a strong platform to ensure a healthy population with access to affordable health care.
Public sector drug procurement is carried out through closed international tenders, Gulf Cooperation Council (GCC) bulk procurement and direct purchasing. The Qatari pharmaceutical market reached a value of Qatari Rial 1.43 billion (US$392.6 million) in 2010. Spending on medicines and pharmaceuticals in 2009 and 2010, as a percentage of total public sector spending, was US$138 million (9%) and US$143 million (8%), respectively [3]. Medicines dispensed at the Hamad Medical Corporation (HMC) health institutions are priced differently for Qataris and non-Qataris. The development of the pharmaceutical market is shaped by the decision of the Supreme Council of Health (SCH) to abolish government controls over the pricing of medicines and to allow more imported goods and suppliers in the country. Qatar has adopted an open market system. The retail prices of medicines remain among the highest in the Middle East.
There is no official policy on the bioequivalence of generic medicines, although the government is promoting their use [3]. Nevertheless, Business Monitor International (BMI) has reported that there is extensive use of branded medicines in Qatar’s healthcare facilities [3]. HMC is using brands mainly because of prescriber’s preference, patient trust and unavailability of a bioequivalence centre in Qatar, where bioequivalence could be studied and tested.
The high share of imported and branded medicines has increased the Qatari government’s healthcare spending. SCH’s attempt to remove price controls affected the affordability of medicines, with the prices of some drugs increasing and becoming inconsistent across facilities. The government has had to implement price controls, although it abstained from explicitly fixing prices.
Qatar’s pharmaceutical market is not able to support its own needs and is likely to remain highly import-dependent, providing significant opportunities for multinational branded drugmakers to penetrate the market. Although the government tends to purchase branded products, the share of the market taken by generic drugs is increasing [3].
There is no national list of approved drugs with therapeutic equivalence, as seen in the US with the Food and Drug Administration’s Orange Book [4]. Anecdotal evidence indicates that, due to preference and cultural aspects, both clinicians and patients prefer to use branded medicines, and the use of generic drugs is low. This has contributed to additional healthcare costs that could have been avoided. Under the National Health Strategy 2011–2016 (Project 5.4), the government has focussed on generic medicines use and awareness in the country. SCH has proposed several behavioural and utilization studies to assess the generic medicines issues among public and healthcare providers, i.e. levels of utilization, perception, knowledge, practice.
It is estimated that the value of Qatar’s drug expenditure at consumer prices in 2009 was Qatari Rial 848 million (US$233 million), having posted double-digit growth in relation to the previous year [5]. Further, according to BMI, prescription drugs continued to dominate the market, accounting for close to 90% of sales by value [5]. By 2014, drug expenditure is forecast to increase by a compound annual growth rate of 11.16%, in both US dollar and local currency terms, as the latter is linked to the former, to reach Qatari Rial 1.44 billion (US$400 million) [5].
The World Bank warns of the impact of poverty and the huge disparity in wealth in the Middle East [6]. Wealthy individuals in the region are needed to invest their resources in projects to reverse this trend, such as by funding pharmaceutical companies to produce generic medicines for the marginalized and poor in the region. In that way, Arabs could bridge the gap between the extremely wealthy and those who lack essential medicines, by removing the reliance on sustained imports of branded medicines. This reliance is currently the case in all Arab countries, especially the six GCC states.
Multinational pharmaceutical companies have been successful in the Qatari market due to high brand consciousness of patients and prescribers for both prescription and over-the-counter medicines. But there is little interest in setting up manufacturing plants in Qatar due to the small market size. Instead, Qatar prefers to import medicines especially from western countries including Europe, UK, USA, and a small proportion from the Middle East and North African countries and Asian countries.
Acknowledgements
The author wishes to thank the English editing support provided by Bea Perks, PhD, GaBI Journal Editor for this manuscript.
Competing interests: None.
Provenance and peer review: Not commissioned; internally peer reviewed.
References
1. National Health Strategy 2011–2016 Supreme Council of Health, Qatar [homepage on the Internet]. [cited 2015 Jan 28]. Available from: http://www.nhsq.info/strategy-goals-and-projects/national-health-policy/healthcare-products-regulation/news-details?item=81&backArt=286
2. General Secretariat for Development Planning of Qatar. Qatar National Vision 2030, Doha, Qatar. July 2008 [homepage on the Internet]. 2008 Jul 27 [cited 2015 Jan 28]. Available from: http://www.gsdp.gov.qa/www1_docs/QNV2030_English_v2.pdf
3. Business Monitor International. Qatar pharmaceuticals & healthcare report Q3 2013. 31 Jul 2013. [cited 2015 Jan 28]. Available from: http://www.rnrmarketresearch.com/qatar-pharmaceuticals-and-healthcare-report-q3-2013-market-report.html
4. U.S. Food and Drug Adminstration. Orange Book: approved drug products with therapeutic equivalence evaluations [homepage on the Internet]. 2015 [cited 2015 Jan 28]. Available from: http://www.accessdata.fda.gov/scripts/cder/ob/
5. Business Monitor International. Qatar pharmaceuticals and healthcare report Q2 2010.
6. Jaber KA. The widening gap between rich and poor in the Arab world. The Peninsula. 20 October 2010. Available from: http://thepeninsulaqatar.com/qatar-perspective/khalid-al-jaber/129823/the-widening-gap-between-rich-and-poor-in-the-arab-world. Accessed 28 January 2015.
|
Author: Professor Mohamed Izham bin Mohamed Ibrahim, PhD, Professor of Social and Administrative Pharmacy, College of Pharmacy, Qatar University, Al Tarfa, PO Box 2713, Doha, Qatar
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2015 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/generic-medicines-policy-in-qatar.html
Copyright ©2024 GaBI Journal unless otherwise noted.
Generics and Biosimilars Initiative (GaBI)
Tel: +32 474989572 | Fax: +32 14 583 048