|
Abstract: |
Submitted: 21 May 2018; Revised: 13 July 2018; Accepted: 17 July 2018; Published online first: 23 July 2018
H.R. 3590 Sec. 7002 [1], commonly known as the Biologics Price Competition and Innovation Act (BPCI Act), a part of the Affordable Healthcare Act, was enacted in 2009 to introduce biosimilars (copies of biological products coming off patent) to the market. Since then, the US Food and Drug Administration (FDA) has licensed 11 products (as of June 2018) [2], comprised of eight molecules: adalimumab, bevacizumab, epoetin, etanercept, filgrastim, infliximab, pegfilgrastim and rituximab. Under the New Drug Application (NDA) filing, insulin glargine products (Lusduna [3] and Basaglar [4]) have also been approved by FDA and from March 2020 all insulin products can be approved as biosimilars [5]. FDA has issued several draft and final guidelines to industry on demonstrating biosimilarity [6], which is the primary determinant for licensing a product, either as a biosimilar or an interchangeable biosimilar. Interchangeable biosimilars are… a separate category of biosimilar products that are additionally tested to demonstrate that automatic substitution of an originator product with the ‘interchangeable biosimilar product’ will not result in reduced efficacy or increased side effects.
The slow entrance and acceptance of biosimilars in the US is the result of high costs and long development times – nearly US$250 million and almost eight years [7] – as well as a gross misunderstanding of the safety of biosimilars among prescribers and the public, principally due to ideas put forward by the products’ originator companies. While FDA has recently launched a campaign to educate stakeholders regarding the safety of biosimilars [8], much work remains to be done in order to simplify and expedite licensing of biosimilars, as emphasized by the author in several publications and a recent citizen petition to FDA [9–11].
The suggestions made in this paper come from decades of experience in developing biosimilar products globally, including through the biosimilars (351(k)) and NDA pathways (505(b)(2)).
This review focuses on actions FDA, biosimilar developers and other stakeholders can take, within the boundaries of the statute, to make biosimilars more accessible. In order to first understand what is feasible for FDA and how the relevant guidelines are constructed, a review of the BPCI Act is necessary. Given below are excerpts from the BPCI Act that are relevant to guidelines for the approval of biosimilars by FDA:
The statutory requirements provided in section k.2.A.i.I form the basis of biosimilar development. Remarkably, these requirements are left to the discretion of FDA, as shown in k.2.A.ii, leaving only section k.2.A.i.I–V as unchangeable by FDA [1]. Interchangeable licensing has additional legislation, as shown in k.4.A–B. A biosimilar product must demonstrate the same clinical results as the reference product, which can only be shown by patient testing. Studies using a switching-and-alternating protocol, where an originator biological product is switched with a biosimilar product and then back to the originator product, must show no diminished efficacy and no greater risk when compared to the reference product without alteration or switching. This legislation prevents FDA from making any changes to the requirements for interchangeable biosimilars; thus this paper will address issues related to the approval of biosimilars only.
To allow the faster development and adoption of biosimilar products, the following changes in the regulatory approval process are recommended:
These recommendations are also, in part, the subject of a citizen petition filed by the author to FDA [11].
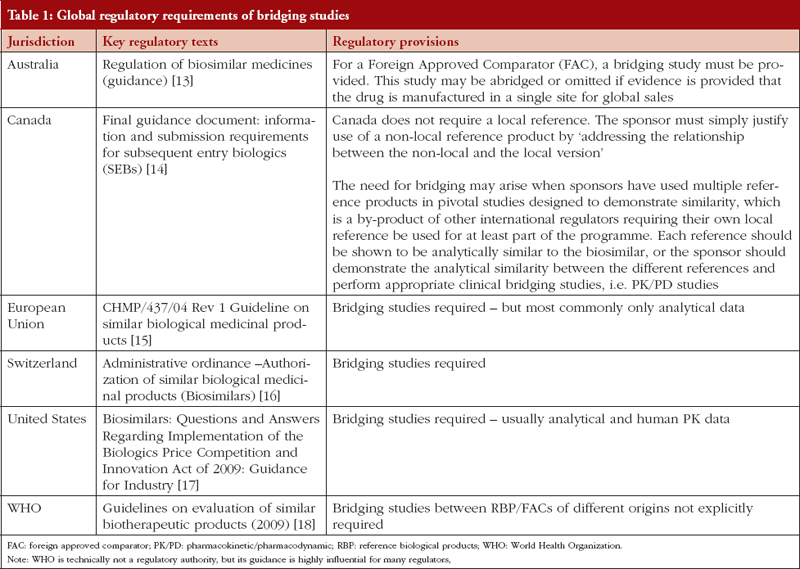
Developing biosimilars is costly and requires developers to formulate a global strategy where one regulatory dossier can be used to secure regulatory approvals in multiple jurisdictions. Since the BPCI Act requires that a biosimilar be similar to its locally licensed originator (that is, a product approved under Sect. 351(a) of the Public Health Service Act of 1942, as amended) [1], developers are not permitted to use a non-US product as a reference product. As a result, creating a global dossier requires three-way studies, i.e. a US-licensed product, a non-US product, and the biosimilar candidate. To reduce the burden of additional studies, and to reduce unnecessary exposure to humans, several regulatory authorities have established clear policies on bridging studies [12], as shown in Table 1.
The most stringent requirements are imposed by FDA, whose requirements include analytical similarity and PK/PD studies. It should be noted that FDA requirements for bridging studies are not clearly defined but accepted as the default position of FDA. As such, there is no legal obstacle to FDA changing its position and allowing developers to request a waiver to use a non-US-licensed product as the reference product, provided the conditions, enumerated below, are met:
FDA Commissioner Dr Scott Gottlieb agrees with the suggestions made above, however, there is wider FDA concern that legislative action would be required to make changes to current practice [21]. The author finds no legal reason why this change cannot be made by FDA.
The BPCI Act creates two categories of biosimilar products: biosimilar and interchangeable biosimilar. The latter classification was intended to allow the automatic substitution of an originator product with a biosimilar product. The labelling of an interchangeable biosimilar requires in patient studies to demonstrate similar efficacy. When a biosimilar product is repeatedly administered, the two products (biosimilar and reference) are alternated to establish that there is no reduction in efficacy or increase in side effects caused by the biosimilar. As a result of the complexity of these studies making them extremely expensive to conduct, developers have been reluctant to file for interchangeable status; and FDA is yet to approve a product as an interchangeable biosimilar. However, there is a need for a strategic approach to allow the substitution of biosimilars based on how FDA characterizes a biosimilar.
‘A biosimilar is a biological product that is highly similar to and has no clinically meaningful differences from an existing the FDA-approved reference product [22]’.
From a scientific and clinical viewpoint, if a product is clinically equivalent, there is no reason why it should not be prescribed to naïve patients. This view is shared by FDA Commissioner Dr Scott Gottlieb who stated that ‘payors can also lead the way in formulary design by making biosimilars the default option for newly diagnosed patients. They can share the savings with patients, maybe by waiving co-insurance [23]’.
The author therefore requests that FDA:
Immunogenicity is defined as the propensity of biological drugs to generate an immune response to self and related proteins, which may include non-clinical effects and adverse clinical events. Immune responses to biological drugs may hamper their biological activities and result in adverse events, not only by inhibiting the efficacy of the therapeutic element but also by cross-reactions with endogenous protein, leading to loss of its physiological function. For example, neutralizing antibodies to erythropoietin can cause pure red cell aplasia by also neutralizing the endogenous protein. The effects of immunogenicity in biological drug development can be summarized as follows:
Immunogenicity, as stated in FDA guidelines on biological drugs, must be assessed in the target population since animal testing and in vitro models cannot predict immune response in humans [24]. Immunogenicity also has a role in demonstrating product comparability following manufacturing changes. Even minor changes can potentially affect the bioactivity, efficacy or safety of a biological drug. As a result, FDA is making important advances in predicting immunogenicity [25], in particular promoting the use of in vitro immunogenicity assays.
The European Medicines Agency (EMA) provides the following statement regarding use of alternate methods of testing immunogenicity:
‘… ongoing consideration should be given to the use of emerging technologies (novel in silico, in vitro and in vivo models), which might be used as tools during development or for the first estimation of risk for clinical immunogenicity. In vitro assays based on innate and adaptive immune cells could be helpful in revealing cell-mediated responses [26]’.
The characterization and screening of biosimilars for physicochemical determinants or formulation-based factors aid both in the prediction of immunogenicity and in the development of less immunogenic therapeutic agents, considering impurities, heterogeneity, aggregate formation, oxidation and deamidation of the molecule. Moreover, predicting potential immunogenic epitopes in therapeutic biologicals is an important and useful strategy to improve their safety.
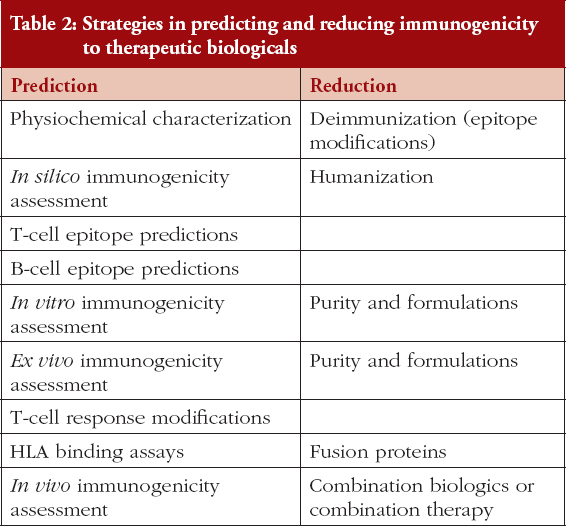
Immunogenicity testing however substantially increases the cost and time requirements for drug development and the goal of regulatory guidance should be to minimize human testing where possible. A variety of preclinical immunogenicity assessment strategies are currently used during biological development, as listed in Table 2.
A major advantage of in vitro methods is the ability to test multiple batches for immunogenicity, which is not possible in human subjects. In vitro tests can also be more useful in predicting the difference between a biosimilar product and its reference product.
There are clear ethical complications in testing for immunogenicity in healthy subjects when comparing a reference drug to a biosimilar candidate. To advance the science of in vitro immunogenicity further, FDA should:
Bioequivalence is defined in 21 CFR 320.1 (Hatch-Waxman Act) [27] as ‘the absence of a significant difference in the rate and extent to which the active ingredient or active moiety in pharmaceutical equivalents or pharmaceutical alternatives become available at the site of drug action when administered at the same molar dose under similar conditions in an appropriately designed study’. Since the site of action is not known in most cases and rarely available for sampling, level in blood was selected as a surrogate to the site of action. The PK profile characterizes two stages, absorption and disposition (distribution and elimination), making it most relevant to generic chemical (small molecule) drugs where disposition is less likely to vary. This makes the PK profile relevant to absorption, and therefore bioavailability, thus providing validation of bioequivalence.
The PK profiling of biosimilars follows the same testing protocols as used for generic drugs. However, extrapolation of testing protocols involves a significant misconception – biosimilar drugs are administered parentally, which means that while differences in absorption are unlikely, differences in disposition are likely (distribution may change due to binding effects for example, and elimination may change due to subtle structural differences). This difference between generics and biosimilars should be addressed in the selection of PK parameters and statistical models applied to demonstrate similarity.
When FDA developed guidance on biosimilars, the term ‘clinical relevance’ was introduced, which is the most crucial aspect of determining biosimilarity and addresses the step-by-step approach [1] of demonstrating: analytical similarity, non-clinical toxicology, PK/PD profile, immunogenicity profile and, if there remains any ‘residual uncertainty’, performing additional clinical studies in healthy subjects. Consideration of ‘clinical relevance’ should therefore also be part of PK/PD analysis.
The author suggests the following changes to the criteria of PK/PD profiling of biosimilars compared to a reference product:
FDA has recently released draft guidance on ‘Statistical Approxaches to Evaluate Analytical Similarity’ for biosimilars [30], one of the most critical components for establishing biosimilarity and a component that determines which additional studies, both clinical and CMC-related, are required. A developer identifies critical quality attributes (CQAs) and tests them using Tier 1, Tier 2, or Tier 3 statistical methods, depending on the nature of data output and the importance of the attribute to the safety and efficacy of a biosimilar product.
For CQAs in Tier 1, equivalence is established by rejecting the interval (null) hypothesis: −1.5 σR ≤ 90% CI of [μT–μR] ≤ 1.5 σ, where μT and μR are the mean responses of the test (the proposed biosimilar product and the reference product lots, respectively). This statistical testing suggests the equivalence acceptance criterion (EAC) = 1.5 × σ, where σ is the variability of the reference product (standard deviation). Statistical justification for the factor of 1.5 [31] follows the idea of the SABE criterion for highly variable generic drug products proposed by FDA. To achieve the desired power for the similarity test, FDA further recommends that an appropriate sample size is selected by evaluating the power using the alternative hypothesis μT − μR = ⅛.
There is no relevance of the factor of 1.5 used in equivalence testing of the most critical CQAs. For example, in the briefing on approval of Sandoz’s filgrastim product [32], FDA stated that one of the CQAs (protein content) initially failed, requiring additional batches to be added to the analyses. While there is a correlation between dose and effect for biological products, a small variation – as observed in the Sandoz data – should not have any clinically meaningful effect, since the release specification provides considerable variability. In essence, a test for analytical similarity may fail, yet such variation is allowed in the commercial product.
The criterion for Tier 1 testing for CQAs can produce misleading results. As an example, 10 batches (a number recommended by FDA) of a biosimilar candidate could be tested against an equal number of reference product batches for a percentage of the labelled quantity of protein. If the variation in the reference product is minimal, approaching a value of zero for σ, then all comparisons will fail, even if there is no clinically meaningful difference. The author has encountered such situations, where an attribute is tightly controlled in the originator product based on decades of manufacturing experience. The question arises if this is a clinically meaningful difference or merely a routine observation. For example, a biosimilar product may be allowed a range of 97–103% or even 95–105% in the Certificate of Analysis (COA) based on the history of manufacturing, yet all samples will fail if the σ of the reference product is minimal. On the other hand, where an attribute has high variability (σ) for the reference product, the product passes the Tier 1 test while failing a Tier 2 test, where 90% of all values fall within 3 × σ. It is for this reason that FDA requires Tier 2 testing for all Tier 1 attributes. To resolve these inconsistencies, the author suggests the following changes to the statistical modelling of CQAs in analytical similarity testing:
It is clearly understood that all analytical methods, including bioanalytical methods, must be validated, as provided in a May 2018 final guidance on bioanalytical methods [33]. However, analytical similarity testing requires methods that are often difficult or impossible to validate based on the guidance provided without incurring high cost and time commitments, such as nuclear magnetic resonance techniques or mass spectrometry. While all analytical methods used in the authorization of a biosimilar should be validated, methods used to demonstrate other analytical attributes may be accepted by FDA if they are ‘suitable’, a term often used in FDA guidance but not clearly defined. There is a need for FDA to clearly differentiate between the methods that must be validated and the ones that can be used if found suitable.
Current approaches to evaluating the differences between a biosimilar candidate and a reference product are based on methods for characterizing new molecules; there is a need to develop more sensitive techniques to determine differences in the structure of large molecules, both at steady state and while active within the body. Several new techniques have recently come into practice, including modified capillary electrophoresis, Chip-based (Bioanalyzer) Protein Electrophoresis Assays (CPEA), and many variations of mass spectrometry [34].
FDA defines fingerprint-like similarity as:
‘the results of integrated, multi-parameter approaches that are extremely sensitive in identifying analytical differences (i.e. fingerprint-like analyses) permit a very high level of confidence in the analytical similarity of the proposed biosimilar product and the reference product, and it would be appropriate for the sponsor to use a more targeted and selective approach to conducting animal and/or clinical studies to resolve residual uncertainty and to support a demonstration of biosimilarity [35]’.
The introduction of new methodologies could help to demonstrate clinically meaningful similarity between products that will reduce the number of additional studies required [36, 37].
Unlike the development of entirely novel drugs, the development of biosimilars requires commercial-scale batches in order to begin testing for similarity. The rationale for this requirement derives from the assumption that there may not be any in patient or ‘phase III’ studies required that are historically conducted using commercial-scale batches. This requirement generates a huge cost and time burden, preventing smaller developers from entering the market. While FDA has not identified what it considers to be ‘commercial scale’, these issues were highlighted in a Type 2 formal meeting between FDA and sponsors of Biosimilar User Fee Act (BsUFA) products [38]. The author suggests that FDA requires a batch size that is adequate to provide samples for stability, clinical or other required testing, instead of making market projections to justify the size of a commercial batch. Should the developer decide to change the batch size after the product has been approved, the developer may use the Comparability Protocol for Biological Drugs [39] to make this post-approval change. This clarification by FDA would have a significant impact on industry, allowing smaller developers to offer market-ready products using smaller batches and at much lower cost.
The largest contributor to the cost and time requirements of marketing a drug are the clinical studies required to establish biosimilarity. When in patient studies are required, the cost and timeline stretch even further. The current mindset of establishing biosimilarity follows phase I to III testing, which is not relevant to establish the non-inferiority status of a biosimilar candidate with the reference product. As a result, the author makes the following recommendations:
In developing methods for the evaluation of biosimilars, FDA has created highly specific vocabulary, such as ‘no clinically meaningful difference’ and ‘residual uncertainty’. These terms are scientifically important and represent a creative approach to assuring the safety of biosimilars. However, not all FDA guidance adequately takes these two terms into account. To improve this situation, this review makes a number of recommendations:
FDA recognizes the need for changes to its guidance. Commissioner Dr Scott Gottlieb [23] has recently expressed a willingness to respond to the urgent need to reinterpret guidelines for the increased approval and adoption of biosimilars.
In June 2018, the FDA withdrew its guidance for Analytical Similarity Testing [40] and a few days later FDA announced a new initiative, Biosimilars Action Plan that includes most of the recommendations made by the author in its citizen petition [41].
This paper represents solely the views of the author and should not be understood or quoted as being made on behalf of or reflecting the position of any regulatory authority or company.
Competing interests: The author of the paper declared that he is a developer of biosimilar products. The author is founder of Karyo Biologics, LLC and Adello Biologics, which have several biosimilar products at various stages of FDA approval.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
1. U.S. Food and Drug Administration. Biologics Price Competition and Innovation Act of 2009. Code of Federal Register. H.R. 3590–687. Title VII—Improving access to innovative medical therapies. Subtitle A—Biologics Price Competition and Innovation [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/drugs/ucm216146.pdf
2. U.S. Food and Drug Administration. Biosimilar product information [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/therapeuticbiologicapplications/biosimilars/ucm580432.htm
3. U.S. Food and Drug Administration. Lusduna: FDA approved drug products [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=208722
4. U.S. Food and Drug Administration. Basaglar (insulin glargine injection) [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/205692Orig1 s000TOC.cfm
5. U.S. Food and Drug Administration. Implementation of the “Deemed to be a License” Provision of the Biologics Price Competition and Innovation Act of 2009 [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM490264.pdf
6. U.S. Food and Drug Administration. Biosimilars guidances [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/Guidances/General/ucm444891.htm
7. Blackstone Erwin A, Fuhr Joseph P, Jr. The economics of biosimilars. Am Health Drug Benefits. 2013;6(8):469-78.
8. Gottlieb S. FDA taking new steps to better inform physicians about biosimilars through education about these potentially cost-saving options. 2017 Oct 23 [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://blogs.fda.gov/fdavoice/index.php/2017/10/fda-taking-new-steps-to-better-inform-physicians-about-biosimilars-through-education-about-these-potentially-cost-saving-options/
9. Niazi S. Obstacles to success for biosimilars in the US market. European Pharmaceutical Review. 2018 Jan 4.
10. Niazi S. eBook: Challenges facing biosimilar entries into US markets. 2018 Jan 16.
11. Niazi S. Citizen Petition from UIC College of Pharmacy. ID: FDA-2018-P-1876-0001.
12. Webester CJ, Woollett GR. A ‘Global reference’ Comparator for biosimilar development. BioDrugs. 2017;31(4):279-86.
13. Australian Government. Department of Health. Therapeutic Goods Administration. Evaluation of biosimilars products [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.tga.gov.au/sites/default/files/pmargpm-biosimilars-150420_1.pdf
14. Government of Canada. Health Canada. Guidance document: information and submission requirements for biosimilar biologic drugs products [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/applications-submissions/guidance-documents/information-submission-requirements-biosimilar-biologic-drugs-1.html
15. European Medicines Agency. Guideline on similar biological medicinal products. CHMP/437/04 Rev 1. 23 October 2014 [homepage on the Internet]. [cited 2018 Jul 13]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2014/10/WC500176768.pdf
16. Swiss Medic. Questions and answers concerning the authorisation of similar biological medicinal products (biosimilars) [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.swissmedic.ch/swissmedic/en/home/legal/legal-basis/administrative-ordinances/questions-and-answers-concerning-the-authorisation-of-similar-bi.html
17. U.S. Food and Drug Administration. Biosimilars: questions and answers regarding implementation of the Biologics Price Competition and Innovation Act of 2009. Guidance for Industry. 2015 April [homepage on the Internet]. [cited 2018 Jul 13]. Available from: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM444661.pdf
18. World Health Organization. Regulatory evaluation of biosimilars throughout their product life-cycle [homepage on the Internet]. [cited 2018 Jul 13]. Available from: http://www.who.int/bulletin/volumes/96/4/17-206284/en/
19. U.S. Food and Drug Administration. FDA briefing document. Arthritis Advisory Committee Meeting February 09, 2016 BLA 125544 CT-P13, a proposed biosimilar to Remicade® (infliximab) Celltrion [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/%E2%80%A6/UCM484859.pdf
20. U.S. Food and Drug Administration. FDA briefing document. Oncologic Drugs Advisory Committee July 13, 2017 BLA 761028 ABP215, a proposed biosimilar to Avastin (bevacizumab) Amgen Inc [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/OncologicDrugsAdvisoryCommittee/UCM566365.pdf
21. Gottlieb: FDA considering an end to biosimilar bridging studies. The Center for Biosimilars. 2018 Feb 16. Available from: http://www.centerforbiosimilars.com/news/gottlieb-fda-considering-an-end-to-biosimilar-bridging-studies-
22. U.S. Food and Drug Administration. Biosimilars and interchangeable products [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/ucm580419.htm
23. U.S. Food and Drug Administration. Gottlieb S. Capturing the benefits of competition for patients [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/NewsEvents/Speeches/ucm599833.htm
24. U.S. Food and Drug Administration. Guidance for Industry. Immunogenicity assessment for therapeutic protein products. 2014 Aug [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/drugs/guidances/ucm338856.pdf
25. U.S. Food and Drug Administration. Immunogenicity of protein-based therapeutics [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/BiologicsBloodVaccines/ScienceResearch/BiologicsResearchAreas/ucm246804.htm
26. European Medicines Agency. Guideline on immunogenicity assessment of therapeutic proteins [homepage on the Internet]. [cited 2018 Jul 13]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2017/06/WC500228861.pdf
27. U.S. Government Publishing Office. CFR: Public Law 98–417–Sept. 24, 1984. Title I–Abbreviated new drug applications [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.gpo.gov/fdsys/pkg/STATUTE-98/pdf/STATUTE-98-Pg1585.pdf
28. European Medicines Agency. Ranizimumab [homepage on the Internet]. [cited 2018 Jul 13]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Scientific_Discussion/human/000715/WC500043550.pdf
29. Niazi S. Volume of distribution as a function of time. J Pharm Sci. 1976;65(3):452-4.
30. GaBI Online – Generics and Biosimilars Initiative. FDA issues draft guidance on statistical approaches to evaluating similarity for biosimilars [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2018 Jul 13]. Available from: www.gabionline.net/Guidelines/FDA-issues-draft-guidance-on-statistical-approaches-to-evaluating-similarity-for-biosimilars
31. Chow SC, Song F, Bai H. Analytical similarity assessment in biosimilar studies. AAPS J. 2016;18(3):670-7.
32. U.S. Food and Drug Administration. FDA briefing document. Oncologic Drugs Advisory Committee Meeting January 7, 2015 BLA 125553 EP2006, a proposed biosimilar to Neupogen® (filgrastim) Sandoz Inc., a Novartis company [homepage on the Internet]. [cited 2018 Jul 13]. Available from: http://patentdocs.typepad.com/files/briefing-document.pdf
33. U.S. Food and Drug Administration. Bioanalytical method validation. Guidance for Industry. 2018 May [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/drugs/guidances/ucm070107.pdf
34. Agilent Technologies. Recombinant protein characterization [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.agilent.com/cs/library/primers/Public/5990-8561EN_LO.pdf
35. U.S. Food and Drug Administration. Clinical pharmacology data to support a demonstration of biosimilarity to a reference product. Guidance for Industry. 2016 Dec [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm397017.pdf
36. Niazi SK. Method for comparing structure of one biomolecule with second biomolecule. United States Pub. No. 2018/0024137 A1. 2018 Jan 25.
37. Niazi SK. Single-use bioreactors and mixing vessels. United States patent 9,469.426 B2. 2016 Oct 18.
38. U.S. Food and Drug Administration. Formal meetings between the FDA and sponsors or applicants of BsUFA products. Guidance for Industry. 2018 Jun [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM609662.pdf
39. U.S. Food and Drug Administration. Comparability protocols for human drugs and biologics: chemistry, manufacturing, and controls information. Guidance for Industry. 2016 Apr [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM496611.pdf
40. U.S. Food and Drug Administration. FDA withdraws draft guidance for industry: statistical approaches to evaluate analytical similarity [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/Drugs/DrugSafety/ucm611398.htm
41. U.S. Food and Drug Administration. Biosimilars Action Plan [homepage on the Internet]. [cited 2018 Jul 13]. Available from: https://www.fda.gov/ucm/groups/fdagov-public/@fdagov-drugs-gen/documents/document/ucm613761.pdf
|
Author: Adjunct Professor Sarfaraz K Niazi, PhD, SI, FRSB, FPAMS, FACB, Adjunct Professor of Biopharmaceutical Sciences, University of Illinois and University of Houston; 20 Riverside Drive, Deerfield, IL 60015, USA |
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2018 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/rationalizing-fda-guidance-on-biosimilars-expediting-approvals-and-acceptance.html
Copyright ©2024 GaBI Journal unless otherwise noted.