Author byline as per print journal: Professor Philip J Schneider1, MS, FASHP, FASPEN, FFIP; Michael S Reilly2, Esq
|
Abstract: |
Submitted: 24 October 2019; Revised: 6 February 2020; Accepted: 17 February 2020; Published online first: 24 February 2020
Introduction
Approximately 25% of all new medicines approved in recent years and in development today are biologicals [1]. The biosimilar market in Europe is the largest in the world, representing approximately 60% of the global biosimilar market and growing consistently year on year [2].
Biosimilars are large and structurally complex molecules obtained from a biological source. Due to inherent biological variability, they can be reproduced to a high degree of – but not complete – similarity [3]. Compared to generics, their development requires additional quality and comparability studies as well as clinical studies on immunogenicity, safety and efficacy [4]. As a consequence, the cost to develop and gain approval for a biosimilar medicine ranges between US$100 million to US$200 million [5].
The European Union (EU) and the European Medicines Agency (EMA) developed a legal framework for the review and development of biosimilars in 2004 [6]. Based on this framework, EMA has a comprehensive set of regulatory guidelines for biosimilar review. One of the most challenging areas in the regulation of biosimilars is switching. So-called ‘switching studies’ where the originator medicine is substituted with the biosimilar candidate and vice versa are not part of the existing European regulatory approval requirements. Neither are studies where biosimilar medicines referencing the same originator medicine are substituted with each other. As a consequence, limited sufficiently powered randomized clinical trial data exist to inform on the risks of switching such as immunogenicity, treatment-emergent adverse events, or lack of efficacy. Because of these factors, the authors of the NOR-SWITCH study recommend caution in generalizing their findings to other biological agents. They also stated that more studies are needed ‘to examine multiple-sequenced as well as back-and-forth switches’ [7].
In summary, a biological medicine should generally not be substituted with another biological or biosimilar medicine that is made using a different bio-manufacturing process. Switching does occur in practice, but the decision to change a patient’s therapy (switch [4]) generally resides with the treating physician in consultation with the patient.
Because of the differences between generic and biosimilar medicines, different rules apply to their clinical use, e.g. procurement practices, prescriber authority and pharmacist involvement. These differences, along with the relative novelty of biosimilars, have resulted in a limited number of biosimilars being made available to date compared with small molecule generics. The limited amount of data available on switching between originator medicines and biosimilars and in-between biosimilars in particular results in a major challenge for all stakeholders – and physicians, patients and payers in particular – to establish policies and frameworks for efficient and patient-friendly long-term sustainable biosimilar markets. These policies must take into consideration: the uniqueness of biosimilar medicines, the educational needs of both physicians and their patients, the maintenance of physician choice and clinical decision-making, the guarantee of drug supply to ensure continuous patient care, pricing rules that do not discriminate against either originator or biosimilar medicines, purchasing mechanisms (procurement frameworks) which encourage companies to compete, and maintaining the correct balance of incentives for providers and prescribers while delivering savings.
Biosimilar competition in Europe
Europe’s legislative and regulatory leadership in biosimilars is evident in European biosimilar sales. While the global biologicals market is dominated by the US, which has a share above 50%, the global biosimilar market has been even more so dominated by the European market, which accounted for close to 90% of global biosimilar sales between 2012 and 2016, see Figure 1.
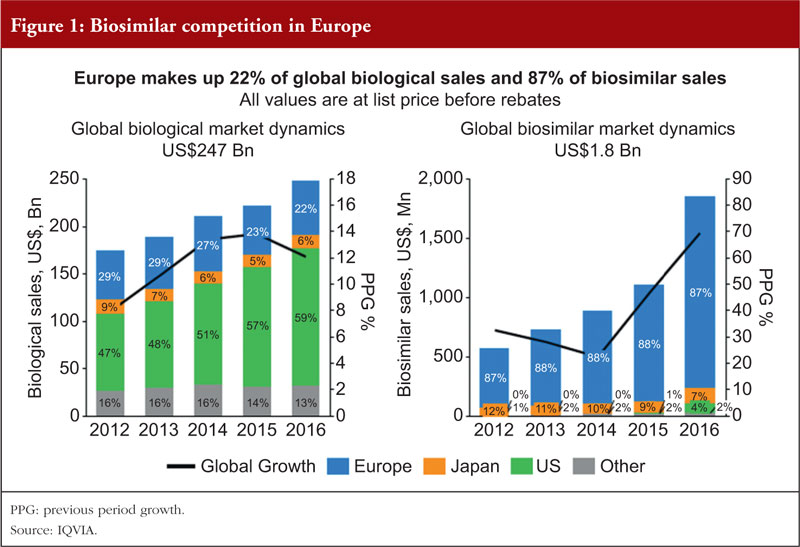
With the launch of 22 biosimilars on the US market since 2017 [8], Europe’s share has been dropping towards 60%, see Figure 1. Although in absolute terms the share of the global biosimilar market as a percentage of the global biologicals market was below 1% in 2016 (compared with 35% of global generics sales as a percentage of global non-biologicals sales), this figure has grown closer to 2.5% and is expected to grow further in the future.
While European biosimilar markets are more mature than those in the US, opportunities for biosimilar companies are smaller in Europe given the overall lower spending on biologicals. In the longer term, the US market represents the greater economic opportunity for these companies [9].
Sustainable biosimilar markets – policy considerations
Several research papers and position statements defining the factors and conditions required for sustainable biosimilar markets have been published in recent years, with the intent to inform policymakers and payers and to support them to develop, assess and refine biosimilar policies in the European Economic Area (EEA, i.e. EU Member States plus Iceland, Liechtenstein and Norway). These publications [10, 14] originate from diverse stakeholders, offering a comprehensive perspective on the necessary conditions for long-term sustainable biosimilar markets, see Appendix 1 on research papers and position statements defining the factors and conditions required for sustainable biosimilar markets in Europe, 2014−2019.
Based on these publications, we believe a ‘gold standard’ for a sustainable European market for off-patent biologicals can be derived, containing six policy requirements:
(1) Policies should be designed to incentivize and reward innovation in all types of biologicals.
(2) Healthcare financing must take into account societal benefits derived from biological medicines, as well as the unique characteristics of biologicals.
(3) Procurement practices must provide for multiple suppliers and a minimum term of 12 months.
(4) Physicians must have autonomy to choose the most appropriate medicine for their patient, including making decisions on switching, which must also be consented to by the patient; no automatic substitution.
(5) There should be mandatory brand- name prescribing to avoid unintended switches as well as a robust pharmacovigilance system to report adverse drug reactions (ADRs).
(6) Policies with potential to undermine sustainability, such as measures which induce biosimilar uptake or promote preferential treatment, thereby limiting physician choice, should be avoided.
When comparing the findings and recommendations from these papers, several key conditions to achieve sustainable biosimilar markets can be identified and may be considered as ‘must haves’ for the long-term success of these markets. These are:
(1) Physicians should have the freedom to choose between off-patent originator biologicals and available biosimilars and to act in the best interest of their patients based on scientific evidence and clinical experience.
(2) Tenders should be designed to include multiple value-based criteria beyond price, e.g. education, services, available dose strengths, and provide a sufficient broad choice (multi-winner tenders versus single-winner tenders) to ensure continuity of supply and healthy competition.
(3) A level playing field between all participating manufacturers is the best way to foster competition; mandatory discounts which place artificial downward pressure on manufacturers do not engender a sustainable market environment.
Elements or conditions recommended by some but not all of the above studies are:
(1) The provision of early access and swift market entry of approved biosimilars upon the innovator’s loss of exclusivity to expand access to treatment for patients while lowering costs.
(2) Incentives, e.g. gainsharing, where a portion of generated savings are returned to prescribers and/or an institution and prescribing targets should be carefully designed so as not to restrict physician choice nor limit competition between originator biologicals and their biosimilars.
(3) The pursuit of a multi-disciplinary team approach when designing payer purchasing policies to ensure the perspectives and needs of different stakeholders, i.e. payers, manufacturers, physicians and patients, are taken into consideration.
(4) Safeguarding the interest of patients and serving their needs as best as possible remains a critical consideration for health authorities, in particular considering the increasing numbers of self-administered biosimilars.
European biosimilar markets – policy examples and experience
Biosimilar policy varies within the 28 EU Member States and the three EEA countries.
Policies have evolved over time and are likely to continue to evolve based on experience, clinical data and the growing number of authorized biosimilars. Current policies are characterized by different supply and/or demand-side incentives as well as different degrees of competition and are determined either at the national, regional or hospital level, or a mixture of these.
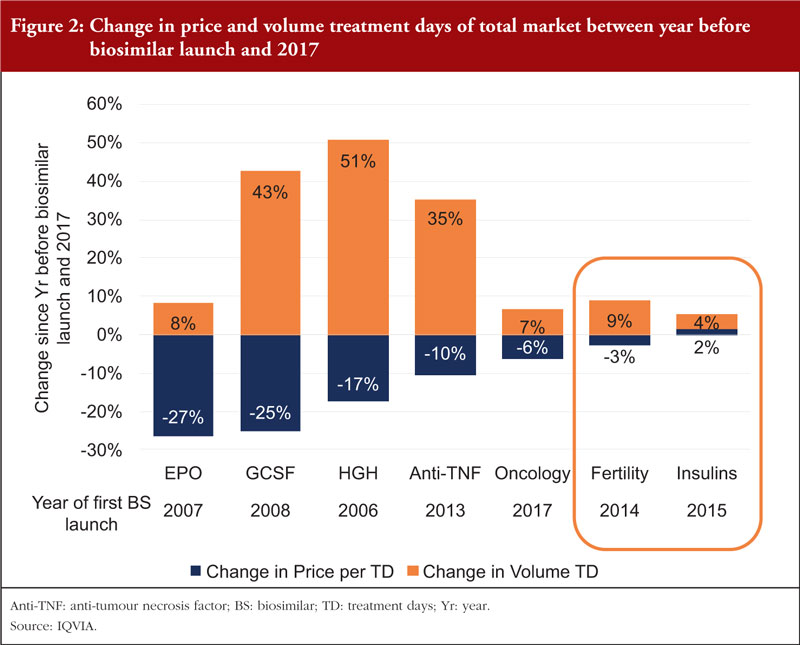
Independent of the kind of policy which is pursued, data suggest that biosimilar price and use also depends on therapeutic area and the time the biosimilar has been on the market. This diversity is reflected in Figure 2, that shows differences in price reductions as well as volume increases for both originator and biosimilar relative to the period prior to when the first biosimilar within a product group was launched [15].
National tender markets
Norway and Denmark are the only European countries to pursue a national tender policy for biosimilar products such as adalimumab, etanercept, or infliximab. Denmark’s policy has been ambitious and restrictive, in that only the manufacturer with the lowest bidding price for a particular molecule will be reimbursed for a 12-month period, potentially requiring physicians to switch patients every 12 months (unless they provide clinical arguments not to do so). In comparison, Norway, which has a history of anti-tumour necrosis factor (anti-TNF) tendering, tenders all molecules in a single tender split by indication as well as application, i.e. infusion or intravenous (IV) (self-administered) based on bi-annual cost according to each product’s prescribing information. Norway then ranks products based on those bi-annual costs in each indication and urges physicians to prescribe the most economical product for new patients. However, the choice is ultimately left to the physician and all lower ranked products are still reimbursed if prescribed, i.e. switching is not explicitly mandated as it is in Denmark. Tenders in Norway tend to be in effect for one year.
Regional and hospital tender markets
In Sweden, hospital administered products are funded by county councils in each of the 21 Swedish counties. Each county runs their own tenders by molecule thus making the market more sustainable for all competitors, as they can compete in more than one tender. Resulting tender prices are communicated among hospital doctors with the intent to promote economic prescribing. As in the case of Norway, all available products continue to be reimbursed if prescribed and, while switching is encouraged, the decision remains with the treating physician and her patient. Tenders tend to run for 24 months and may be re-opened as new competitors enter the market. A recent study of infliximab prescribing in Sweden [16] showed that biosimilar infliximab prescribing varied between regions depending on the absolute difference in price between the originator and the biosimilar products, the opinion of key opinion leaders and clinic heads, local guidelines and hospital initiatives.
With the intent to increase competition, maintain choice for physicians and their patients and avoid shortages of supply from a single manufacturer, Italy passed a national law in December 2016 (2017 Budget Law) which forbids automatic substitution in the case of biologicals and gives priority to the physician’s freedom of prescription. Based on this law, if there are no more than three suppliers of a specific molecule on the market, each is available to physicians to be prescribed. In cases where there are more than three suppliers, the three lowest priced products may be prescribed. In both cases, prices are determined in hospital tenders for both IV and subcutaneous (SC) products in each of the Italian regions. For stable patients, physicians may choose to continue the current treatment under the condition that the respective medicine participated in the tender process.
As in Sweden, hospital tenders in France only apply to IV products. Tenders tend to promote a single winner based on price with a duration of 12 months. Physicians are encouraged to prescribe the most economical product for new patients as well as for stable patients, even though the decision to switch a patient is left at the physician’s discretion. However, while a single switch from the originator to a considerably lower priced biosimilar is seen as less controversial, multiple switches are looked upon unfavourably, unless a very substantial discount to the previously lowest priced biosimilar applies. Given that hospitals are paid a lump sum per patient per case, lower priced products offer a profit incentive to hospitals.
In Spain, similar to Italy, hospitals tender both IV and SC products by molecule, all products remain available for physicians to choose from, and all products are reimbursed. In addition to hospital tenders, some regions have pursued biosimilar prescribing targets, however, physicians’ responsibility to provide the best treatment for their patients remains paramount. Furthermore, physicians are liable for their treatment choices as regards patient outcomes.
In Poland, medicines are prescribed in the hospital. Every hospital is obliged to tender each molecule annually and only the winning bidder can generally expect to be used and reimbursed during each 12-month tender period. As a result, competition has been particularly fierce, and the longer-term sustainability of the biosimilar market may be affected. In addition, product choice for physicians and their patients is limited, both for new and stable patients.
In the UK, National Health Service (NHS) England in their September 2017 publication ‘Commissioning framework for biological medicines (including biosimilar medicines)’ stated that ‘… at least 90% of new patients will be prescribed the best value biological medicine within three months of launch of a biosimilar medicine, and at least 80% of existing patients within 12 months, or sooner if possible’. In England, which comprises 80% of UK citizens, NHS England has provided guidance in their Commissioning Framework for Biological Medicines. Based on tenders in each of the four regions within England, prices for originators and their biosimilars are determined for both IV and SC products. Commissioners are encouraged to promote switching where appropriate, incentivize prescribing and monitor biosimilar uptake. While all approved biologicals remain available for prescribing by physicians, various mechanisms have been put in place to promote the use of the best value biological medicine [17].
Retail and hospital contract markets
Germany, where both SC and IV biologicals are primarily prescribed by private doctors, is the largest retail market in Europe. Pricing is free allowing for price competition both at the list price level as well as towards individual sick funds based on discount agreements. German Statuary Health Insurance (GKV), which represents dozens of health insurers and the German National Association of Statutory Health Insurance Physicians (KBV), agrees national prescription volume targets for biosimilars. However, such quotas vary widely by region and molecule, as regional associations are not obliged to abide by national targets and are free to set higher or lower regional targets. To achieve set quotas, private doctors’ prescribing practices are monitored to encourage compliance. Despite these incentives, physicians remain free in their choice among all available products and are expected to base their decision on clinical data, experience and patient needs. All available products are reimbursed. For biologicals prescribed in the hospital, prices are typically determined by contracts agreed between hospitals and manufacturers.
In France, SC biologicals are prescribed by private doctors and reimbursed nationally. While certain quotas do apply, similar to Germany, French physicians are free to choose the best product for their patients and all available products are reimbursed.
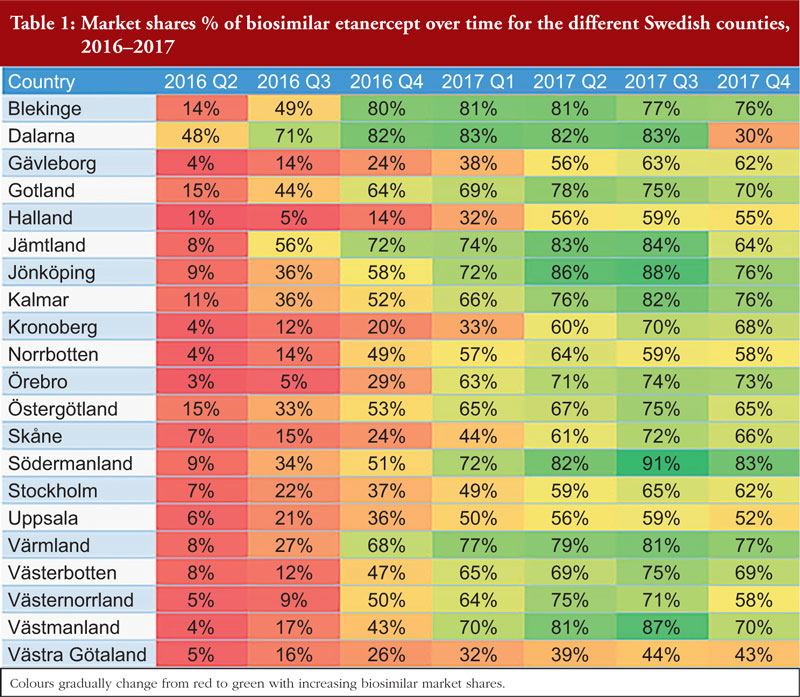
In Sweden, hospital tenders apply only to IV products, but SC biologicals are prescribed in the hospital and reimbursed centrally. Prices for SC biologicals are determined in so-called managed entry agreements by way of three-party negotiations between The Dental and Pharmaceutical Benefits Agency, county councils and manufacturers. After an agreement is reached, prices apply nationwide. Managed entry agreements have durations of up to two years and may be re-visited when new competitors arrive. Savings resulting from these agreements are shared between the government (40%) and the counties (60%). Physicians are free to prescribe the most suitable product for their patients while taking economic arguments into consideration. Based on two recent studies of infliximab and etanercept in Sweden [16], see Table 1, biosimilar prescribing varied between regions to a larger degree in the case of infliximab probably due to a limited price difference between originator and biosimilar etanercept in comparison with infliximab. Overall, as in the case of infliximab, etanercept volume has increased, likely driven by a lower threshold to prescribe and by higher and more appropriate dosing.
Solution
Understanding, acceptance, familiarity and use of biosimilars in Europe have evolved in recent years. Based on 13 years’ experience with biosimilars in off-patent biologicals markets in Europe, it can be stated that biosimilars have: (1) increased competition; (2) reduced unit cost of both originator and biosimilars compared to price levels prior to the arrival of biosimilars; (3) increased volume consumption of molecules with biosimilar competition thus expanding market access and optimizing patient dosing; and (4) alleviated budget pressures by providing headroom to fund novel treatment solutions.
While the policies by which this has been achieved vary between countries, all major European markets share the following principles:
(1) Automatic substitution for biologicals is forbidden.
(2) All approved biologicals, i.e. originators and their biosimilars, are available on the market and are reimbursed when prescribed.
(3) Reimbursement decisions on novel treatment solutions are independent from biosimilar use and uptake.
(4) The time from market approval to first product sales for biosimilars is shorter than the time to first sales of novel medicines [18].
Biosimilars have attained market shares in some European markets as high as 91% for older products (before the approval of the first monoclonal antibody biosimilar in 2013) and as high as 43% for newer products (approved post-2013) [15]. However, this does not necessarily mean that countries with a more moderate biosimilar market share are less competitive. On the contrary, these markets tend to benefit not only from the use of lower cost biosimilars but equally from lower cost originators. Furthermore, markets with multiple manufacturers tend to be better positioned for the long term since market participation and price levels allow for a return on investment which will accommodate the development and launch of future biosimilars, the generation of real-world data and more patient-friendly devices and services. Last but not least, such markets allow physicians to choose among available products and act in the best interest of their patients based on clinical evidence, experience and patient preferences.
As countries decide on their biosimilar policies, they must strike the right balance between a desire for substantial immediate savings and more sustainable savings in the long term, as well as future innovations. The number of future off-patent biologicals offers an attractive savings outlook which should not be jeopardized by a short-term race to the bottom of the prices of today’s biosimilars. Policymakers should carefully design procurement measures such as tenders and contracting to ensure: (1) a wide and non-discriminatory choice of products; (2) selection criteria beyond price such as services and supply; (3) the avoidance of (forced) multiple switches [19]; and (4) the involvement of physicians, pharmacists and other stakeholders in the process. Any demand-side incentives to promote biosimilar prescribing, such as biosimilar market share targets, financial prescriber incentives or sanctions, should also be designed with care regarding their size and level of enforcement in order to ensure appropriate product use. This ultimately needs to be a clinical decision made by the treating physician for an individual patient on the basis of shared decision-making.
Conclusions
Creating a new market is a slow process. It took the generics sector over a decade to establish itself as the major volume driver in developed markets. After more than a decade of biosimilar experience in Europe, biosimilars have gained wider acceptance and the use of newly approved products has increased. While many blockbuster products with European sales above US$1 billion have lost market exclusivity during this decade, there will only be three such products going off patent in the decade to come. The majority of products will have sales between US$100 million to US$1 billion [20]. For future off-patent originator biologicals to offer a compelling investment for multinational biosimilar companies, regulatory and payer policies which help to foster a fair and sustainable environment will be crucial. Advocacy from patient and industry groups as well as healthcare providers will be important to convince market gatekeepers to develop a market with these characteristics.
The European experience is testament to the value of multi-stakeholder participation and engagement at every stage of the process, from the regulatory framework through education all the way to procurement policy decisions and treatment guidelines. Trust is at the core of matters such as the appropriate use of complex medicines for the treatment of chronic and life-threatening diseases; only an approach which is transparent and includes all stakeholders will facilitate the long-term acceptance of biosimilar products.
In their pursuit of savings and increased patient access in off-patent biologicals markets, stakeholders will need to strike the right balance between both short- and long-term savings, as well as the maintenance of patient care and physician and patient trust. Based on the European experience to date, the most suitable policies appear to be those which provide continuous, unbiased information on biosimilars, stimulate manufacturer competition, guarantee a sufficiently broad choice of products, are non-discriminatory towards either originator or biosimilar medicines and allow the treating physician to choose the most appropriate product in consultation with their patient. Given the required investment to develop a biosimilar medicine, their market access and participation should be supported by medical guidelines and incentives such as prescribing targets for biosimilars. While the use of biosimilars for bio-naïve patients is not controversial, some uncertainty remains about switching patients currently being treated with an originator product to a biosimilar (or vice versa), from one biosimilar to another, and about switching on multiple occasions [21]. Any incentives must take these uncertainties into account in order for prescriber and patient confidence in biosimilar medicines to evolve.
Funding sources
This paper is funded by the Alliance for Safe Biologic Medicines (ASBM).
The ASBM is an organization composed of diverse healthcare groups and individuals – from patients to physicians, innovative medical biotechnology companies and others – who are working together to ensure patient safety is at the forefront of the biosimilars policy discussion. The activities of ASBM are funded by its member partners who contribute to ASBM’s activities. Visit www.SafeBiologics.org for more information.
Competing interests: Professor Philip J Schneider is a member of the International Advisory Board of Alliance for Safe Biologic Medicines (ASBM) since 2012 without compensation. From September 2014, Emeritus Professor Schneider has been the Chair of the International Advisory Board of ASBM and is paid a small stipend for that role. Mr Michael S Reilly, Esq, is the Executive Director and employed by Alliance for Safe Biologic Medicines. Mr Reilly served in the US Department of Health and Human Services from 2002–2008.
Provenance and peer review: Not commissioned; externally peer reviewed.
Authors
Professor Philip J Schneider1, MS, FASHP, FASPEN, FFIP
Michael S Reilly2, Esq, Executive Director
1College of Pharmacy, The Ohio State University, 500 West 12th Avenue, Columbus, OH 43210, USA
2Alliance for Safe Biologic Medicines, PO Box 3691, Arlington, VA 22203, USA
References
1. Will biologics surpass small molecules in the pharma race? BiopharmaTrend.com. 2018 July 11.
2. IQVIA. MIDAS MAT Q4 2018. Middle East & Africa pharmaceutical market insights [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.iqvia.com/-/media/iqvia/pdfs/nemea/mea/edition-13-mea-pharmaceutical-market-quarterly-report.pdf
3. European Commission. Biosimilars in the EU: a paradigm in regulatory science [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://ec.europa.eu/docsroom/documents/38050
4. European Medicines Agency. Biosimilars in the EU, Information guide for healthcare professionals, 2017. [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.ema.europa.eu/en/documents/leaflet/biosimilars-eu-information-guide-healthcare-professionals_en.pdf
5. Belloni A, Morgan D, Paris V. Pharmaceutical expenditure and policies: past trends and future challenges. 2016. OECD Health Working Papers, No. 87, OECD Publishing, Paris.
6. European Commission. Directive 2001/83/EC, as amended by Directive 2003/63/EC and Directive 2004/27/EC
7. Jørgensen KK, Olsen IC, Guro L, Goll GL, Lorentzen M, Bolstad N, et al. Kvien TK, on behalf of the NOR-SWITCH study group. Switching from originator infliximab to biosimilar CT-P13 compared with maintained treatment with originator infliximab (NOR-SWITCH): a 52-week, randomised, double-blind, non-inferiority trial. The Lancet. 2017;389(10086):2304-16.
8. U.S. Food and Drug Administration. FDA-approved biosimilar products 10 [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.fda.gov/drugs/biosimilars/biosimilar-product-information
9. IQVIA, The global use of medicine in 2019 and outlook to 2023, January 2019 [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.iqvia.com/insights/the-iqvia-institute/reports/the-global-use-of-medicine-in-2019-and-outlook-to-2023
10. Medicines for Europe. Factors supporting a sustainable European biosimilar medicines market [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.medicinesforeurope.com/wp-content/uploads/2016/03/GfK_Final_Report-_Factors_Supporting_a_Sustainable_European_Biosimilar_Medicines_Market.pdf
11. European Federation of Pharmaceutical Industries and Associations. EFPIA policy principles for off-patent biologic medicines in Europe [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://efpia.eu/media/15409/efpia-policy-principles-for-off-patent-biologic-medicines-in-europe-september-2015.pdf
12. Medicines for Europe. Simon Kucher & Partners. Payers’ price & market access policies supporting a sustainable biosimilar medicines market [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.medicinesforeurope.com/wp-content/uploads/2016/09/Simon-Kucher-2016-Policy-requirements-for-a-sustainable-biosimilar-market-FINAL-report_for-publication.pdf
13. IQVIA. Advancing biosimilar sustainability in Europe [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.iqvia.com/insights/the-iqvia-institute/reports/advancing-biosimilar-sustainability-in-europe
14. European Federation of Pharmaceutical Industries and Associations. Towards a sustainable European market for off-patent biologics [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://efpia.eu/media/412909/towards-a-sustainable-european-market-for-off-patent-biologics-pugatch-consilium.pdf
15. European Commission. IQVIA. The impact of biosimilar competition in Europe. September 2018 [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://ec.europa.eu/docsroom/documents/31642
16. Moorkens E, Simoens S, Troein P, Declerck P, Vulto AG, Huys I. Different policy measures and practices between Swedish counties influence market dynamics: Part 1—Biosimilar and originator infliximab in the hospital setting. BioDrugs. 2019;33:285-97.
17. National Health Service England. Commissioning framework for biological medicines. September 2017 [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.england.nhs.uk/wp-content/uploads/2017/09/biosimilar-medicines-commissioning-framework.pdf
18. IQVIA. Advancing biosimilar sustainability in Europe [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.iqvia.com/institute/reports/advancing-biosimilar-sustainability-in-europe
19. Scherlinger M, Schaeverbeke T. ‘To switch or not to switch’: the missing piece in the puzzle of biosimilar literature? Ann Rheum Dis. 2019;pii: annrheumdis-2018-214908.
20. Arias A. Future biosimilars opportunities. 2019 [homepage on the Internet]. [cited 2020 Feb 6]. Available from: https://www.iqvia.com/blogs/2019/12/future-biosimilar-opportunities
21. Simoens S, Le Pen C, Boone N, Breedveld F, Celano A, Llombart-Cussac A, et al. How to realize the potential of off-patent biologicals and biosimilars in Europe? Guidance to policymakers. Generics and Biosimilars Initiative Journal (GaBI Journal). 2018;7(2):70-4. doi: 10.5639/gabij.2018.0702.014
Appendix 1: Research papers and position statements defining the factors and conditions required for sustainable biosimilar markets in Europe, 2014−2019
In 2014, consultancy GfK Market Access published a study undertaken on behalf of the European Generics Association (EGA) now Medicines for Europe on Factors supporting a sustainable European biosimilar medicines market [10]. In this study, four elements for a Sustainability Policy Framework were identified, namely: (1) Education and Understanding; (2) Experience and Use; (3) Sustainable Pricing; and (4) Rational Decision-making. The core considerations under each of these elements were:
(1) Education and Understanding
- Improved understanding of accurate unbiased information about biosimilar medicines
- Awareness and understanding of the requirements for a sustainable biosimilar market
(2) Experience and Use
- Encouragement and incentives for physicians for early appropriate use, e.g. thoughtful implementation of quotas that do not undermine physicians’ prescribing choice; ‘gainsharing’ arrangements where a proportion of savings in a hospital is returned
(3) Sustainable Pricing
- Policies which encourage free and fair competition on a level playing field which do not undermine continued investment
- Avoidance of arbitrary, prescriptive pricing policies, e.g. mandatory discounts, that place artificial downward pricing pressure on manufacturers
(4) Rational Decision-making
- Recognition of the value of differentiated product offerings, e.g. drug delivery, services, dose strengths as well as outcomes data (economic, clinical and disease management)
- Procurement policies involving multiple stakeholders, including physicians, offering a choice of therapies available for patients
- Avoidance of exclusive (single winner) tendering policies to maintain competition, product choice and to mitigate potential supply risks
In 2015, the European Federation of Pharmaceutical Industries and Associations (EFPIA) published their Policy principles for off-patent biologic medicines in Europe [11] ‘to help healthcare systems to design and implement policies that can successfully create competitive off-patent biological markets’. The four principles identified by EFPIA and the core aspects in each of them were:
(1) Overarching principles for European off-patent biological markets
- Biologicals including biosimilars are not the same as small molecules including generics and policies must be designed specifically for them
- The prescribing physician should always have the option to designate which biological product should be dispensed to the patient
(2) Principles for creating sustainable competition
- Competition should create a level playing field and be non-discriminatory towards either originator or biosimilar medicines
- Early and sustained market access and entry of biosimilars
(3) Principles for prescribing frameworks
- The decision to switch patients from one biological product to another can only be made by the treating physician accompanied by clinical monitoring and prior information of the patient
- Pharmacy-level substitution is not an acceptable practice for biological medicines as long as they are not designated as being substitutable by the competent regulatory authority
(4) Principles for specific market mechanisms
- Purchasing and procurement practices must always involve a medical committee
- The design of tenders should contain a variety of selection criteria and not only focus on price, guarantee supply and continuation of treatment by providing a sufficient broad choice of products and avoid a ‘winner takes all’ scenario
- If implemented, uptake measures like quotas and financial incentives/sanctions must not restrict physician choice nor limit competition in a discriminatory manner against either type of product, i.e. originator biological or biosimilar
In 2016, consultancy Simon & Kucher published a report undertaken on behalf of Medicines for Europe titled Payers’ price & market access policies supporting a sustainable biosimilar medicines market [12]. In their comprehensive study based on data and interviews with payers and manufacturers, Simon & Kucher identified the following principles for a sustainable biosimilar medicines market:
(1) Biosimilars increase competition thus increasing access for more patients and funding for new innovative medicines
(2) Pricing and procurement policies should ensure continuous market participation of several manufacturers to maintain healthy competition
(3) Biosimilar policies should allow physicians to choose from different treatment alternatives
- Single-lot tenders limit physicians’ flexibility and choice
- No pharmacy-led automatic substitution; the physician should always have the option to designate which biological product should be dispensed to the patient
(4) Tender decisions should not be based only on price. They should take into consideration multiple value-based influencing factors, e.g. supply, education, services
(5) Procurement policies should allow parallel sourcing to sustain competition and supply
(6) Pricing and procurement policies for biosimilar markets must be commercially attractive to sustain competition and biosimilar investment long term
(7) Pricing and market access policies enforcing lower prices (compared to their originators) have to be accompanied by specific guidance on biosimilar use and prescribing incentives
(8) Voluntary and mandatory price discounts without volume compensation do not offer biosimilar manufacturers a sustainable market environment
(9) Gainsharing is considered a successful driver of biosimilar uptake
(10) Physician incentive policies are only sustainable if payers monitor physicians’ policy adherence
In 2018, pharmaceutical consultancy IQVIA published the multi-stakeholder assessment Advancing Biosimilar Sustainability in Europe [13], which was commissioned and funded by Pfizer. In this assessment IQVIA identified five key areas that have significant influence on the sustainability in the biosimilar marketplace: the current regulatory environment, clinical guidelines for biosimilars, product and supply features, incentives for biosimilar use and competitive market pressures such as pricing. Based on an analysis of policies in seven EEA countries (France, Germany, Italy, Norway, Poland, Spain, UK), the following key sustainability elements emerged:
(1) Regulatory environment and clinical guidelines favourable to biosimilar approval and uptake
(2) Guidelines and policies supporting a physician-guided therapy switch
(3) Prescription freedom for physicians enabling them to select therapy for patients, i.e. no automatic substitution
(4) Availability of multiple products, enabling physicians’ choice of approved therapies
(5) Well-designed incentives that foster biosimilar uptake, while safeguarding physician choice and patient input into treatment decisions, such as treatment switch
(6) Consideration of the long-term sustainability of the market as well as physician needs when designing incentives to facilitate budget release
(7) Incentivize biological manufacturers towards continued patient-friendly innovation
(8) Balance price pressures of payer purchasing mechanisms with requirements for long-term market sustainability; implement policies that address the needs of all market stakeholders
(9) Sustain healthy competition with multi-winner tenders as compared with single-winner tenders
(10) Sustain healthy product supply by enabling access for both originator and biosimilar products
In 2019, boutique consultancy Patch Consilium published the study Towards a sustainable European market for off-patent biologics [14] which was commissioned and funded by EFPIA. The objective of this study was to assess how policy and governance frameworks should be designed and implemented to ensure long-term sustainable off-patent biological markets through an analysis of the current policy ecosystem in 15 EEA countries (Belgium, Czech Republic, France, Germany, Greece, Hungary, Italy, Netherlands, Norway, Poland, Romania, Slovakia, Spain, Sweden, UK) regarding the pricing environment, procurement practices and the degree of physician autonomy and patient choice and through a survey among different stakeholders in these countries regarding their perceptions of the off-patent biologicals. The core findings are summarized below:
(1) Pricing environment
- Seven countries use external reference pricing to achieve the lowest price from a large basket of reference countries
- Eight countries condition the biosimilar market entry on a mandatory price reduction at a pre-defined percentage from the originator product’s price
(2) Procurement practices
- The majority of countries base procurement practices solely on price and some of them limit treatment choices through single-winner tenders
- With 12 months or less, tender frequency is too high in several countries in Europe
(3) Physician autonomy and patient choice
- Physicians are offered incentives for prescribing biosimilars in 13 European countries
- Automatic substitution is allowed in the Czech Republic, Estonia, Latvia and Poland
(4) Stakeholder* perception
- Physician prescribing autonomy, access to a range of available treatments and access to reliable and up-to-date information were the top three most important requirements for a sustainable biologicals off-patent market
*Stakeholders interviewed were: Healthcare Professionals, Patients/Patient Group Representatives, Government Institution Representatives and Industry/Trade Association Representatives; due to the limited number of responses (76) and uneven distribution between stakeholders, the study states that they may not reflect the common view of these stakeholder groups.
|
Author for correspondence: Michael S Reilly, Esq, Executive Director, Alliance for Safe Biologic Medicines, PO Box 3691, Arlington, VA 22203, USA |
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2020 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.