Comment on the article by Reilly MS and McKibbin RD
|
Abstract:
Reilly and McKibbin oppose the update of FDA interchangeability guidance that does not require clinical switch studies. However, their arguments lack a scientific basis.
|
Submitted: 3 December 2024; Revised: 17 December 2024; Accepted: 18 December 2024; Published online first: 18 December 2024
Comment on the article by Reilly MS and McKibbin RD: Misinformation about interchangeable biosimilars undermines US health policy, physician confidence, and patient health.GaBI Journal, 2024;13(2):55-60.
The US Food and Drug Administration (FDA) has updated its guidance on interchangeability [1]. It now states that the risk in terms of safety or diminished efficacy is insignificant following single or multiple switches between a reference product and a biosimilar product. Therefore, it proposes that clinical interchangeability (switch) studies are not required for automatic substitution. If implemented, the interchangeability designation will become obsolete. Updated guidance is a rational step in the evolution of the biosimilar concept in the USA. It also increases possibilities to harmonize regulatory requirements globally which is necessary to fully exploit the full potential of biosimilars. Furthermore, the updated guidance will mitigate the confusion and misunderstandings concerning interchangeability among prescribers, patients, and policymakers globally.
The proposed new policy followed a large and thorough review and meta-analysis of safety and immunogenicity switching studies by experts of FDA [2]. The results were in line with several previous reviews of the safety, efficacy, and immunogenicity of switches between originators and their biosimilars.
The article of Reilly and McKibbin [3], representing the Alliance for Safe Biological Medicines – a coalition of patient advocacy organizations – presents harsh criticism of the study of FDA experts and opposes proposals to abandon clinical switch studies currently required for interchangeability designation. Their arguments are based on opinions, perceptions, beliefs, and fundamental misunderstandings of the ability of randomized clinical trials to detect differences of proteins shown to be highly similar in terms of structure, function, immunogenicity, efficacy and safety.
Reilly and McKibbin admit that FDA-approved biosimilars are indisputably safe and effective medications and the physician may choose to prescribe either to their patient, whether naïve or stable. Furthermore, they state that all FDA-approved biosimilars may be substituted in place of the reference product by the physician. Thus, the core of the matter is the passing of prescribers in selection of the brand of therapeutically equivalent products and the removal of clinical switch studies from the FDA guidance. The authors refer to surveys showing that many prescribers are reluctant to switch from originator to its biosimilars. Surveys and opinion polls have also demonstrated that physicians have limited knowledge of the relevant literature and the underlying science as well as of the economic impact of biosimilars. Prescribers’ expectations of the role of randomized clinical trials in the demonstration of potential small differences between biosimilars and originator products are unrealistic.
The authors ignore previous large review articles of clinical switching studies [2]. These studies suggest that single or repeated switches between originators and biosimilars or between biosimilars of the same originator do not have significant adverse effects on efficacy, safety and immunogenicity. Thus, potential switch-related differences are rare or very small after a single or repeated switches. Randomized clinical trials cannot detect these potential problems.
In 2019, when the first FDA guidance was published, there was limited experiences of repeated switches. As a result, FDA decided to require a clinical study with three consecutive switches to detect a potential immunological boosting effect that could lead to adverse effects. In this context, clinical efficacy endpoints were too insensitive to detect decreased efficacy in a meaningfully sized clinical study. Instead, changes in immunogenicity and pharmacokinetics were used as surrogates for efficacy. However, even with a reasonable sample size, the sensitivity for detecting these changes remained poor [4].
Despite the current understanding of the limitations of randomized clinical switch studies, Reilly and McKibbin argue that, without conducting switching studies, it is unknown whether efficacy diminishes or if side effects arise more frequently following a switch. They also ignore the review and meta-analysis of the FDA experts and previous reviews on the safety, efficacy and immunogenicity of switches. They go even further and complain about the lack of studies in different therapeutic indications and patient populations. In the absence of clear signals of switch-related adverse effects, these claims are invalid from the scientific and regulatory point of view. Considering the current state of knowledge, continuation or even expansion of the current switch studies would be unethical and an unnecessary burden to patients and industry.
The authors statement that the automatic substitution of biosimilars at the pharmacies in the US would represent a dramatic contrast to European practices is misleading. There is a common scientific definition of interchangeability in the EU that is not in conflict with the prosed guidance of FDA [5]. In contrast, EU Member States have adopted a variety of practical measures that are based on the common scientific definition, such as automatic substitution, regional or national tendering, prescription quotas, and price control according to national legislation and the structure of health care.
Ironically, the title of the article of Reilly and McKibbin is ‘misinformation about interchangeable biosimilars undermines US health policy, physician confidence, and patient health’. I fully agree with this statement.
Funding sources
No funding was received to write this letter.
Disclaimer
The author alone is responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which he is affiliated.
Competing interests: The author declares no conflicts of interest.
Provenance and peer review: Not commissioned; internally peer reviewed.
References
1. US Food and Drug Administration. Considerations in demonstrating interchangeability with a reference product: update June 2024 [homepage on the Internet]. [cited 2024 Dec 17]. Available from:https://www.fda.gov/regulatory-information/search-fda-guidance-documents/considerations-demonstrating-interchangeability-reference-product-update
2. Herndon TM, Ausin C, Brahme NN, Schrieber SJ, Luo M, Andrada FC, et al. Safety outcomes when switching between biosimilars and reference biologics: a systematic review and meta-analysis. PLoS ONE. 2023;18(10):e0292231.
3. Reilly MS, Ralph D McKibbin RD. Misinformation about interchangeable biosimilars undermines US health policy, physician confidence, and patient health. Generics and Biosimilars Initiative Journal (GaBI Journal). 2024;13(2):55-60. doi:5639/gabij.2024.1302.009
4. Alvarez DF, Wolbink G, Cronenberger C, Orazem J, Kay J. Interchangeability of biosimilars: what level of clinical evidence is needed to support the interchangeability designation in the United States? BioDrugs. 2020;34(6):723-32. doi:10.1007/s40259-020-00446-
5. European Medicines Agency. Statement on the scientific rationale supporting interchangeability of biosimilar medicines in the EU [homepage on the Internet]. [cited 2024 Dec 17]. Available from:
https://www.ema.europa.eu/en/documents/public-statement/statement-scientific-rationale-supporting-interchangeability-biosimilar-medicines-eu_en.pdf
|
Author: Adjunct Professor Pekka Kurki, MD, PhD, University of Helsinki, Lukupolku 19, FI-00680 Helsinki, Finland
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2025 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/letter-to-the-editor-to-comment-the-article-reilly-ms-and-mckibbin-rd.html
Comparative efficacy studies of biosimilars: data versus theoretical risks, beliefs, and comfort
|
Abstract:
In principle, biosimilars could mitigate the problem of the rising cost of biological medicines. However, the current stringent and non-harmonized regulatory practices hinder competition and contribute to the high price level of biosimilars. The quality, safety, and efficacy of biosimilars developed, according to the current guidelines of ‘stringent’ regulatory agencies have proven to be excellent. Analytical and in vitro functional testing combined with clinical pharmacokinetic and pharmacodynamic studies provide the essential data to prove the similarity of candidate biosimilars to their reference products. The standard in vivo non-clinical toxicological studies are useless, and the value of ‘confirmatory’ controlled efficacy (and safety) trials have been questioned by several independent retrospective studies of current biosimilars, including monoclonal antibodies and fusion proteins. Thus, the development of biosimilars could be streamlined to lower costs without increasing risks to efficacy or safety of products. The UK regulatory agency, Medicines and Healthcare products Regulatory Agency (MHRA), and the World Health Organization (WHO) have recently revised their biosimilar guidelines to allow the development of biosimilars without ‘confirmatory’ clinical efficacy studies when the biosimilar candidate can be thoroughly characterized and shown to be structurally and functionally similar to the reference product that has no unpredictable serious adverse effects. The European Medicines Agency (EMA) is already exploring possibilities to revise its guidance accordingly. Unfortunately, the US Food and Drug Administration (FDA) is still hesitating. The US guidance should be revised to remove the interchangeability studies and reduce the controlled efficacy trials. Otherwise, the global biosimilar market will not be able to provide better access to biological medicines.
|
Submitted: 8 April 2024; Revised: 18 April 2024; Accepted: 19 April 2024; Published online first: 29 April 2024
Introduction
Biological therapies are rapidly advancing scientifically. Gene and cell therapies have already entered the clinic. However, the success story of biologicals is overshadowed by the high costs that are increasingly limiting access to life-saving medicines [1].
The costs of chemically synthesized medicines dramatically drop following the introduction of generic equivalents, after the exclusivity period. Biosimilars are copies of biologicals that can also, in principle, reduce the costs of off-patent biologicals. Unfortunately, biosimilars have not succeeded in fulfilling their potential. There are several reasons for their poor performance.
The unwillingness of prescribers to prescribe and switch to biosimilars has delayed the growth of the biosimilar market. Resistance remains despite availability of scientific and educational publications on the safety and efficacy of biosimilars. It seems obvious that the hesitance is due to non-scientific reasons such as misinformation, administrative burden, worries about physician autonomy, and lack of incentives [2]. Therefore, several countries have adopted or are planning to adopt automatic substitution policies and tendering to promote rational use of biologicals.
The other main reason for the high prices of biosimilars is lack of competition caused by two main factors. Namely, these are the anti-competitive measures put in place by the innovator industry, such as questionable patents, and the stringent regulatory requirements for biosimilars leading to high development costs [3–5]. The regulatory guidelines for biosimilars in the European Union, US and elsewhere were initially very conservative. They have been revised over time but remain stringent. The main factors contributing to the high development costs include purchasing the reference comparator biological products and running controlled efficacy trials with large patient samples to demonstrate clinical equivalence. The stringent regulatory requirements are expected to constrain the ability of current manufacturers to develop biosimilars needed for rare diseases, and new manufacturers to develop products and join the competition [4]. This paper aims to clarify as what is already known about the role of large clinical efficacy studies and the ongoing re-evaluation of their future role in biosimilar development.
The role of large efficacy and safety studies in biosimilar development
The current guidelines of European Medicines Agency (EMA) and US Food and Drug Administration (FDA) allow some flexibility in designing the clinical development of biosimilars but in practice, a comparative efficacy trial with clinical efficacy endpoint can only be avoided by conducting a pharmacodynamic (PK) study with a marker that is an established surrogate of efficacy. Such pharmacodynamic (PD) markers are not available for most biosimilars, notably monoclonal antibodies (mAbs). This means that, without revision of the guidelines, even more efficacy studies will be conducted in future as most new biosimilars will be mAbs or their derivatives. Thus, controlled efficacy studies are not only expensive but will also strain the clinical research resources of hospitals which may delay the development of new innovative medicines, especially in oncology.
Long-term safety of biosimilars
At the inception of biosimilar guidelines and products, there were many uncertainties. The long-term safety and efficacy of biosimilars has been surprisingly good, considering their current widespread use. None of the theoretical worries, including issues related to immunogenicity and extrapolation of therapeutic indications, have yielded post-licensing issues [6–9]. Thus, the development concept of biosimilars has been validated. The remaining question is whether all parts of the development; analytical, in vitro functional tests, in vivo non-clinical models, human PK and PD studies, as well as comparative efficacy and safety studies, provide useful information. Analytical and in vitro functional testing, as well as clinical PK/PD studies do provide unique information, whereas the in vivo non-clinical toxicology studies are considered useless [7]. Comparative efficacy (and safety) studies have been called ‘confirmatory’ but are increasingly controversial.
Are large efficacy/safety studies necessary?
The conduct of clinical efficacy and safety studies is regarded as the gold standard in the development of new innovative medicines. The requirement of comparative clinical efficacy studies in the development of biosimilars is deeply rooted in the minds of many clinicians and regulators. Several retrospective studies have been conducted to estimate the impact of efficacy studies on the approvability of biosimilars [10–15]. The studies covered all products approved 2006–2019 [10, 11] or focused on the more complex molecules, mAb and fusion proteins [12–14]. Data were extracted from public assessment reports, mainly from the European Public Assessment Reports. It was revealed that controlled efficacy studies did not significantly contribute to the regulatory decision-making process and that they are insensitive to significant analytic and in vitro functional differences. In general, products that were comparable in analytical, in vitro functional, and PK studies were approved irrespectively of the outcome of the comparable efficacy study.
There were two cases of increased immunogenicity due to leachables from the syringe epoetin-α and host cell impurities (somatropin). These problems can be avoided in the future as our experience of developing and evaluation of biosimilars has increased. The performance of analytical methods and our understanding of structure function relationships have improved over time. Differences in the active substances did not trigger significant differences in immunogenicity between the biosimilar and the reference product.
There were two cases where the candidate biosimilar was rejected due to a lack of analytical comparability, even though the clinical efficacy study met the equivalence criteria. There were three products that were comparable in analytical and in vitro functional tests and/or PK study but the comparative efficacy study failed to demonstrate equivalence. In these cases, post hoc analyses of the efficacy data led to the approval. In conclusion, comparative efficacy studies do not significantly affect regulatory decision-making. Thus, it is doubtful whether clinical efficacy studies can be called ‘confirmatory’ for biosimilarity because of their lower sensitivity for significant differences. Post-marketing surveillance is the only feasible way to detect rare serious adverse effects.
Confirmatory efficacy studies: are regulatory dominos falling?
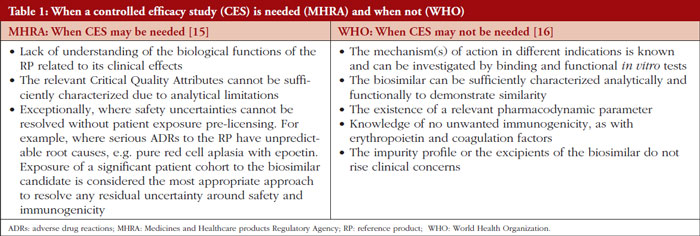
UK regulatory agency Medicines and Healthcare products Regulatory Agency (MHRA) and the World Health Organization (WHO) have revised their biosimilar guidelines by listing factors that may justify the conduct of a powered efficacy study [15, 16]. Using these criteria, manufacturers may ask for a waiver of the comparative efficacy study, see Table 1. It is expected that, using these criteria, comparative efficacy studies will be exceptional in the development of conventional biosimilar therapeutic proteins. Thus, the goal is not the categorical elimination of controlled efficacy studies, especially in development of new types of complex biosimilars or proteins that have serious unpredictable adverse effects.
EMA’s Biosimilar Medicines Working Party (BMWP) of the Committee of Human Medicinal Products (CHMP) has issued a concept paper that proposes drafting a reflection paper for re-evaluation of the need for comparative efficacy studies [17]. Several former and current BMWP experts have published scientific articles supporting the reduction of comparative efficacy studies and some participated in drafting the WHO guideline. [13, 14, 16, 18] Thus, it would be surprising if the reflection paper would not recommend the revision of the CHMP guidelines according to the current knowledge of the role of powered efficacy studies in the development of biosimilars.
FDA appears to be the most conservative major regulatory agency. FDA has a rather flexible guidance concerning comparative efficacy trials in biosimilar development, but it has been applied in a conservative manner. The interchangeability designation is an additional hurdle, as it may be difficult to reduce comparative efficacy studies if companies must conduct large comparative switching studies to obtain the designation. The main clinical concern of FDA seems to be immunogenicity. FDA experts published a thorough review of interchangeability studies [19]. The conclusion was that no difference was found in the safety profiles or immunogenicity rates in patients who were switched and those who remained on a reference biological. This study, together with several previous reviews, questions the scientific and ethical justification of switch studies.
FDA hosted a workshop of The Biosimilar Working Group of International Pharmaceutical Regulators Programme (IPRP) in September 2023, to discuss the need for comparative efficacy studies in biosimilar development [20]. Regulators representing ‘stringent’ agencies had a broad agreement in the need for re-evaluation of the role of comparative efficacy studies, but no concrete international consensus efforts were proposed. WHO and MHRA presented their models for reducing comparative efficacy studies. EMA announced the ongoing process for revision of its guidance on comparative efficacy studies. FDA had more reservations which were explained by the ‘newness’ of the biosimilar concept and the difficulty of reversing the strong historical attachment to comparative efficacy studies — the gold standard for innovative medicines. In addition, FDA seems not to be entirely convinced in the extrapolation of historical evidence to future biosimilars. Instead, FDA has a research programme aiming to find innovative ways to simplify biosimilar development, such as biomarkers, PD markers, new statistical methods, testing drug formulations, and better understanding of the clinical significance of differences in the analytical and in vitro functional tests, as well as possibilities to predict immunogenicity by in silico and in vitro methodologies [21]. These efforts may benefit the development of biological medicines in general. However, the finding and validation of the potential new methods for demonstration of biosimilarity may take years.
Pharmaceutical regulation should serve public health
Some medicines regulatory agencies are streamlining their requirements while others are hesitating. Experts from the biosimilar industry argue that the necessary data for revision and harmonization of regulatory guidance are already available [22]. This situation raises increasing concerns among payers and policymakers in the US and elsewhere about increasing costs of biological therapy. In fact, the US budget proposal for 2025 includes a legislative initiative to ‘Eliminate the Statutory Distinction between the Approval Standard for Biosimilar and Interchangeable Biosimilar Products and Deem that Approved Biosimilars are Interchangeable’ [23]. This would be in line with the statement of EMA and the Heads of Medicines Agencies in the EU and might pave the way for reduction of comparative efficacy studies.
According to the pharmaceutical legislation in the EU, the essential aim of the regulation of medicinal products must be to safeguard public health [24]. However, this goal must be attained by means which will not hinder the development of the pharmaceutical industry or trade in medicinal products within the Community. These principles fit well in the discussion about comparative efficacy studies. Increased competition will lead to better access to important medicines and removal of redundant efficacy studies will allow new companies to initiate biosimilar development.
It is obvious that the reduction of comparative efficacy studies would trigger criticism among parts of the industry that are afraid of increasing competition. Prescribers are used to relying on comparative efficacy studies and have still difficulties in understanding the concept of biosimilarity. Thus, they may be shocked if the ‘confirming’ (in fact comforting) comparative efficacy studies are not required anymore for all biosimilars. Therefore, regulators need to ally with learned societies that have issued position papers on biosimilars and have the authority to explain the data on the true role of ‘confirmatory’ efficacy studies. Even then, automatic substitution may become necessary to speed up the acceptance of the revised biosimilar development concept.
Many important therapeutic proteins have recently lost the exclusivity or will lose it soon [25]. Thus, regulators should not miss the opportunity to simplify and accelerate the development of new biosimilars. EMA and FDA should strive to a common or at least compatible position with WHO and MHRA on the role of comparative efficacy studies and the interchangeability concept. This would increase harmonization of key regulatory requirements without an arduous ICH-type harmonization process.
Disclaimer
The author alone is responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which he is affiliated.
Funding sources
No funding was received to write this article.
Competing interests: The author declares no conflicts of interest.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
1. Makurvet FD. Biologics vs. small molecules: drug costs and patient access. Med Drug Discov. 2021;9:100075.
2. Sarnola K, Merikoski M, Jyrkkä J, Hämeen-Anttila K. Physicians’ perceptions of the uptake of biosimilars: a systematic review. BMJ Open. 2020;10(5):e034183.
3. Chen BK, Yang YT, Bennett CL. Why biologics and biosimilars remain so expensive: despite two wins for biosimilars, the Supreme Court’s recent rulings do not solve fundamental barriers to competition. Drugs. 2018;78(17):1777-81.
4. IQVIA. Assessing the biosimilar void achieving sustainable levels of biosimilar competition in Europe. 2023 [homepage on the Internet]. [cited 2024 Apr 18]. Available from:https://www.iqvia.com/insights/the-iqvia-institute/reports-and-publications/reports/assessing-the-biosimilar-void
5. Fontanillo M, Körs B, Alex Monnard A. Three imperatives for R&D in biosimilars. McKinsey & Company. 19 August 2022. Available from: https://www.mckinsey.com/industries/life-sciences/our-insights/three-imperatives-for-r-and-d-in-biosimilars
6. Kurki P, Barry S, Bourges I, Tsantili P, Wolff-Holz E. Safety, immunogenicity and interchangeability of biosimilar monoclonal antibodies and fusion proteins: a regulatory perspective. Drugs. 2021;81(16):1881-96.
7. Kurki P, Kang HN, Ekman N, Knezevic I, Weise M, Wolff-Holz E. Regulatory evaluation of biosimilars: refinement of principles based on the scientific evidence and clinical experience. BioDrugs. 2022;36(3):359-71.
8. Nikitina V, Santi Laurini G, Montanaro N, Motola D. Comparative safety profiles of oncology biosimilars vs. originators in Europe: an analysis of the EudraVigilance Database. Cancers (Basel). 2023;15(14):3680.
9. Sagi S, Anjaneya P, Kalsekar S, Kottke A, Cohen HP. Long-term real-world post-approval safety data of multiple biosimilars from one marketing-authorization holder after more than 18 years since their first biosimilar launch. Drug Saf. 2023;46(12):1391-404.
10. Webster CJ, Wong AC, Woollett GR. An efficient development paradigm for biosimilars. BioDrugs. 2019;33:603-11.
11. Schiestl M, Ranganna G, Watson K, Jung B, Roth K, Capsius B, et al. The path towards a tailored clinical biosimilar development. BioDrugs. 2020;34(3):297-306.
12. Bielsky MC, Cook A, Wallington A, Exley A, Kauser S, Hay JL et al. Streamlined approval of biosimilars: moving on from the confirmatory efficacy trial. Drug Discov Today. 2020:S1359-6446(20)30343-3.
13. Guillen E, Ekman N, Barry S, Weise M, Wolff-Holz E. A data driven approach to support tailored clinical programs for biosimilar monoclonal antibodies. Clin Pharmacol Ther. 2023;113(1):108-23.
14. Kirsch-Stefan N, Guillen E, Ekman NV, Barry S, Knippel V, Killalea S, et al. Do the outcomes of clinical efficacy trials matter in regulatory decision-making for biosimilars? BioDrugs. 2023;37:855-71.
15. Medicines & Healthcare products Regulatory Agency. Guidance on the licensing of biosimilar products. 2022 [homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://www.gov.uk/government/publications/guidance-on-the-licensing-of-biosimilar-products/guidance-on-the-licensing-of-biosimilar-products
16. World Health Organization. Guidelines on evaluation of biosimilars. Replacement of annex 2 of WHO technical report series, no.977. 2022 [homepage on the Internet]. [cited 2024 Apr 18]. Available from:https://www.who.int/publications/m/item/guidelines-on-evaluation-of-biosimilars
17. European Medicines Agency. Concept paper for the development of a Reflection Paper on a tailored clinical approach in biosimilar development [homepage on the Internet]. [cited 2024 Apr 18]. Available from:https://www.ema.europa.eu/en/documents/other/concept-paper-development-reflection-paper-tailored-clinical-approach-biosimilar-development_en.pdf
18. Wolff-Holz E, Tiitso K, Vleminckx C, Weise M. Evolution of the EU biosimilar framework: past and future. BioDrugs. 2019;33(6):621-34.
19. Herndon TM, Ausin C, Brahme NN, Schrieber SJ, Luo M, Andrada FC, et al. Safety outcomes when switching between biosimilars and reference biologics: a systematic review and meta-analysis. PLoS One. 2023;18(10):e0292231.
20. U.S. Food and Drug Administration. IPRP Biosimilars Working Group Workshop: ‘Increasing the efficiency of biosimilar development programs re-evaluating the need for comparative Clinical Efficacy Studies (CES)’13 September 2023 [homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://www.fda.gov/media/172198/download
21. U.S. Food and Drug Administration. BsUFA III Regulatory Research Pilot Program: Research Roadmap [ homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://www.fda.gov/media/164751/download
22. Cohen HP, Turner M, McCabe D, Woollett GR. Future evolution of biosimilar development by application of current science and available evidence: the developer’s perspective. BioDrugs. 2023;37(5):583-93.
23. U.S. Food and Drug Administration. FY25 Legislative proposals [homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://www.fda.gov/media/176924/download?attachment
24. EUR-Lex. Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001 on the Community code relating to medicinal products for human use [homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32001L0083
25. Troien P, Newton M, Scott K, Mulligan C. The impact of biosimilar competition in Europe. IQVIA Report 2021. Available from: https://www.iqvia.com/-/media/iqvia/pdfs/library/white-papers/the-impact-of-biosimilar-competition-in-europe-2021.pdf
|
Author: Adjunct Professor Pekka Kurki, MD, PhD, University of Helsinki, 19 Lukupolku, FI-00680 Helsinki, Finland
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2024 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/comparative-efficacy-studies-of-biosimilars-data-versus-theoretical-risks-beliefs-and-comfort.html
No need for systematic switch studies to demonstrate interchangeability of biosimilars
|
Abstract:
Systematic clinical switch studies to demonstrate interchangeability of biosimilars are required in some jurisdictions while theoretical considerations and current clinical data question the feasibility and relevance of such studies.
|
Submitted: 27 November 2021; Revised: 15 December 2021; Accepted: 15 December 2021; Published online first: 28 December 2021
Biosimilars have been used for 15 years in the European Union (EU). They are able to trigger price competition and reduce costs as well as to increase access to important biological medicines [1]. In spite of the long experience and excellent safety record, many prescribers and other healthcare professionals still have concerns about the quality, safety, efficacy, and especially interchangeability of biosimilars [2]. Systematic clinical switch studies to demonstrate interchangeability of biosimilars are required in some jurisdictions while theoretical considerations and current clinical data question the feasibility and relevance of such studies.
Differences in terminology and regulatory approach hurt biosimilars
In the EU, interchangeability is a scientific and clinical concept meaning that switching between a biosimilar and its reference product does not change the efficacy or safety [3]. Interchangeable products can be switched under the control of the prescriber (physician-led switch) or at the pharmacy without consultation of the prescriber (automatic substitution). Both scenarios are practical applications of interchangeability. Several European national regulatory authorities have issued position papers that endorse physician-led switching [4]. Automatic substitution is a political, administrative, and practical measure that may require changes to the legislation and needs to be adapted to local circumstances.
In the US, interchangeability is regarded as a higher level of biosimilarity that allows automatic substitution. The US Food and Drug Administration (FDA) may grant interchangeable status to already licensed biosimilars if they fulfill the requirements of its interchangeability guideline [5]. The main hurdle is the conduct of a controlled clinical trial consisting of three switches. The switch studies constitute a significant burden to developers and patients. In addition, the results may not give a definite answer [6]. Thus far, the interchangeable status has been granted to only two products by FDA; Semglee (insulin glargine-yfgn) in July 2021 and Cyltezo (adalimumab-adbm) in November 2021.
In spite the fact that switch studies are not required in the EU, the concept a clinical switch study is deeply rooted in the minds of prescribers and policymakers also in the EU, as seen in some position papers of national regulatory authorities and learned societies [4] and in the hesitance among prescribers [2]. Manufacturers whose old blockbuster products are threatened by biosimilars support requirements for systematic multiple switch studies and even switch studies between biosimilars and repeated demonstration of interchangeability [7-9] – obviously because extensive switch studies discourage biosimilar development. The feasibility of conducting extensive switch studies has been questioned [6, 10]. Moreover, it is difficult to find detailed theoretical justifications and clinical data to support systematic switch studies. Thus, the crucial question is not what kind of comparative switch studies should be done but whether these studies are justified and feasible at all.
The hypothesis of switch-related immunogenicity
Immunogenicity is presented as the risk of switching between a biosimilar and its reference product. The FDA interchangeability guideline states,‘in the context of switching between the products, multiple exposures to each product may potentially prime the immune system to recognize subtle differences in structural features between products’ and‘the overall immune response could be increased under these conditions’ [5]. Some proponents of switch studies explain this hypothesis by the discontinuation theory [7]. Thus,‘subtle’ differences in the structure, notably the glycosylation profiles of active substances of biosimilars and their reference product seem to be a cornerstone for the immunogenicity hypothesis [8]. This theory may be relevant to vaccines that are designed to be‘foreign’ to human immune system and immune response is amplified by adjuvants ― a completely different situation compared to therapeutic proteins that are made highly similar. Thus, this possibility is also highly unlikely after switching between a biosimilar and its reference product that have already been shown to be highly similar and which are expected to have some degree of immunological tolerance due to their resemblance to human proteins [11].
It is also suggested that exposure to different sets of antigenic epitopes upon switching might enhance anti-drug immunity by epitope spreading. This situation has been observed in epoetin alpha (epoetin-α) products where a poor product formulation or inappropriate storage may lead to cross-reacting neutralizing antibodies to endogenous erythropoietin. The root cause of the induction of neutralizing erythropoietin antibodies is aggregation of proteins in a poor formulation [12]. Thus far, there is no clinical data to support above-mentioned immunogenicity theories in the context of switching between a reference product and its licensed biosimilar version.
Switch-related immunogenicity: a remote risk
Switch-related immunogenicity is often seen as an unpredictable reaction of the immune system. However, the factors triggering of anti-drug immunity are well known. Immune recognition is essential for identifying proteins as‘self’ or‘non-self’. Recognition of the protein as‘non-self’ may be associated with transient or persistent immune reactions. The switching between highly similar versions of the same active substance is not sufficient to break tolerance and to raise persisting and strong T cell-dependent immunogenicity such as affinity maturation, isotype switch or strong recall response due to the identical amino acid sequence and highly similar secondary structure. Differences in glycosylation profiles have never triggered immunogenicity of different versions of therapeutic proteins [10]. Such differences are found after changes in manufacturing process and even between different batches of therapeutic proteins without immunological problems [13]. Studies of originator and biosimilar infliximab and adalimumab support the similarity of important antigenic epitopes in biosimilars and their reference products [14-16].
B cells may be stimulated independently by impurities, such as bacterial endotoxins as well as by degraded and aggregated proteins [11]. Such problems may be due to inappropriate storage or poor formulations, i.e. not due to‘subtle differences’ in the active substances of highly similar products in normal use. These cases, such as the formulation change of originator epoetin-α or one of its biosimilar versions have made developers and regulators very careful in assessing formulations and stability studies of biosimilars [17]. Therefore, it is unlikely that licensed biological products will have immunogenicity triggered by impurities [13].
The clinical evidence
Review of 178 clinical switch studies of biosimilars and their reference products found no evidence of switch-related adverse effects, including harmful immunogenicity [18]. More recent reviews of newer biosimilars confirm the lack of switch-related adverse effects [19, 20]. From a theoretical perspective, the lack of adverse effects is the expected outcome whereas the hypothesis of switch-related adverse effects is not supported by current evidence [6, 11, 21]. Furthermore, clinical switch studies will not be able to detect potential rare adverse effects. Thus, the risk management of switching should be based on pharmacovigilance and pharmaco-epidemiological studies.
Clinical switch studies: time for a re-evaluation
The concept of systematic switch studies is becoming obsolete, but FDA keeps requiring extensive studies due to US legislation. The innovative industry is promoting even more extensive switch studies due to their commercial interests, experts do not dare to challenge FDA and the existing dogma, and prescribers are confused. Ironically, a similar situation has been described in the old tale‘The Emperor’s New Clothes’ [22].
The moral of the tale of systematic switch studies is that EU regulators should have the courage to issuing a common position in interchangeability of biosimilars [23]. The message should be that EU-licensed biosimilars are interchangeable with its reference product without systematic clinical switch studies.
Funding sources
No financial support was received for conducting this research.
Disclaimer
The opinions expressed in this article are personal views of the author and should not be understood being made on behalf of or reflecting the position of the agencies or organizations with which the author is or has been affiliated.
Competing interests: None.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
1. Troein P, Newton M, Scott K. The impact of biosimilar competition in Europe. December 2020 [homepage on the Internet]. [cited 2021 Dec 15]. Available from: https://ec.europa.eu/health/sites/health/files/human-use/docs/biosimilar_competition_en.pdf
2. Barbier L, Simoens S, Vulto AG, Huys I. European stakeholder learnings regarding biosimilars: Part I—improving biosimilar understanding and adoption. BioDrugs 2020;34:783-96.
3. European Medicines Agency and European Commission. Biosimilars in the EU. Information guide for healthcare professionals [homepage on the Internet]. [cited 2021 Dec 15]. Available from: https://www.ema.europa.eu/en/documents/leaflet/biosimilars-eu-information-guide-healthcare-professionals_en.pdf
4. Medicines for Europe. Positioning statements on physician-led switching for biosimilar medicines. 2020 [homepage on the Internet]. [cited 2021 Dec 15]. Available from: https://www.medicinesforeurope.com/docs/M-Biosimilars-Overview-of-positions-on-physician-led-switching.pdf
5. U.S. Food and Drug Administration. Considerations in demonstrating interchangeability with a reference product. Guidance for Industry. May 2019 [homepage on the Internet]. [cited 2021 Dec 15]. Available from: https://www.fda.gov/media/124907/download
6. Alvarez DF, Wolbink G, Cronenberger C, Orazem J, Kay J. Interchangeability of biosimilars: what level of clinical evidence is needed to support the interchangeability designation in the United States? BioDrugs. 2020;34(6):723-32.
7. Faccin F, Tebbey P, Alexander E, Wang X, Cui L, Albuquerque T. The design of clinical trials to support the switching and alternation of biosimilars. Expert Opin Biol Ther. 2016;16(12):1445-53.
8. Feagan BG, Marabani M, Wu JJ, Freddy Faccin F, Spronk C, Castañeda-Hernández G. The challenges of switching therapies in an evolving multiple biosimilars landscape: a narrative review of current evidence. Adv Ther. 2020;37(11):4491-518.
9. Afzali A, Furtner D, Melsheimer R, Molloy PJ. The automatic substitution of biosimilars: definitions of interchangeability are not interchangeable. Adv Ther. 2021;38(5):2077-93.
10. Mysler E, Azevedo VF, Danese S, Alvarez D, Iikuni N, Ingram B, et al. Biosimilar-to-biosimilar switching: what is the rationale and current experience? Drugs. 2021;81(16):1859-79.
11. Doevendans E, Schellekens H. Immunogenicity of innovative and biosimilar monoclonal antibodies. Antibodies (Basel). 2019;8(1):21.
12. Rubic-Schneider T, Kuwana M, Christen B, Aßenmacher M, Hainzl O, Zimmermann F, et al. T-cell assays confirm immunogenicity of tungsten-induced erythropoietin aggregates associated with pure red cell aplasia. Blood Adv. 2017;1(6):367-79.
13. Lamanna WC, Holzmann J, Cohen HP, Guo X, Schweigler M, Stangler T, et al. Maintaining consistent quality and clinical performance of biopharmaceuticals. Expert Opin Biol Ther. 2018;18(4):369-79.
14. Reinisch W, Jahnsen J, Schreiber S, Danese S, Panés J, Alejandro Balsa A, et al. Evaluation of the cross-reactivity of antidrug antibodies to CT-P13 and infliximab reference product (Remicade): an analysis using immunoassays tagged with both agents. BioDrugs. 2017;31(3):223-37.
15. Ben-Horin S. Yavzori M, Benhar I, Fudim E, Picard O. Ungar B, et al. Cross-immunogenicity: antibodies to infliximab in Remicade-treated patient with IBD similarly recognise the biosimilar Remsima. Gut. 2016;65(7):1132-8.
16. Goncalves J, Myung G, Park M, Jeong D, Ghil J. SB5 shows cross-immunogenicity to adalimumab but not infliximab: results in patients with inflammatory bowel disease or rheumatoid arthritis. Therap Adv Gastroenterol. 2019;12:1756284819891081.
17. European Medicines Agency. Guideline on similar biological medicinal products containing biotechnology-derived proteins as active substance: quality issues (revision 1). 22 May 2014 [homepage on the Internet]. [cited 2021 Dec 15]. Available from:https://www.ema.europa.eu/en/documents/ scientific-guideline/guideline-similar-biologicalmedicinal- products-containing-biotechnologyderived- proteins-active_en-0.pdf
18. Barbier L, Ebbers H, Declerck P, Simoens S, Vulto A, Huys I. The effi cacy, safety, and immunogenicity of switching between reference biopharmaceuticals and biosimilars: a systematic review. Clin Pharmacol Ther. 2020;108(4):734-5.
19. Strand V, Gonçalves J, Hickling TP, Jones HE, Marshall L, Isaacs JD. Immunogenicity of biosimilars for rheumatic diseases, plaque psoriasis, and infammatory bowel disease: a review from clinical trials and regulatory documents. BioDrugs. 2020;34(1):27-37.
20. Kurki P, Barry S, Bourges I, Tsantili P, Wolff- Holz E. Safety, immunogenicity and interchangeability of biosimilar monoclonal antibodies and fusion proteins: a regulatory perspective. Drugs. 2021;81(16):1881-96.
21. Chamberlain P. Multidisciplinary approach to evaluating immunogenicity of biosimilars: lessons learnt and open questions based on 10 years’ experience of the European Union regulatory pathway. Biosimilars. 2014;4:23-43.
22. Andersen HC. The emperor’s new clothes (“Kejserens nye klæder”). In: Reitzel CA. Fairy tales told for children. Third Booklet. 1837.
23. Ebbers HC, Schellekens H. Are we ready to close the discussion on the interchangeability of biosimilars? Drug Discov Today. 2019;24(10):1963-7.
|
Author: Adjunct Professor Pekka Kurki, MD, PhD, University of Helsinki, 19 Lukupolku, FI-00680 Helsinki, Finland
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2022 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/no-need-for-systematic-switch-studies-to-demonstrate-interchangeability-of-biosimilars.html
EU Member States have tools to reduce costs of bestseller biologicals but can they use them?
|
Abstract:
Major cost savings are achievable in pharmacotherapy in the European Union since biosimilars to most best-selling biological medicinal products have been licensed. Unfortunately, the window of opportunity may be missed since neither national pricing, reimbursement and procurement systems nor prescribers are well prepared for biosimilars’ entry to the market.
|
Submitted: 9 March 2018; Revised: 11 March 2018; Accepted: 12 March 2018; Published online first: 23 March 2018
Introduction
Biosimilars to most blockbuster biologicals have now been licensed in the European Union (EU). The key biologicals have estimated sales of Euros 40 billion in 2016–2020 in the main European markets [1]. Thus, the healthcare systems in the EU will soon get a relief provided by great savings and a better access to important medicines – or maybe not?
The problem is that EU Member States do not have a common master plan or shared idea as how to collect the reward for having biosimilars approved. Decisions for interchangeability, price, reimbursement, procurement and instructions to prescribers are made separately in each Member State [2]. The final decisions to use biosimilars are usually made by individual hospitals and prescribers. By each step, different decisions are made. Because of this highly complicated situation, biosimilars have had a very modest and variable success in penetrating the markets dominated by originator products. At the moment, prescribers are the main gatekeepers for biosimilars into the health care.
Prescribers suffer from lack of knowledge and motivation
In spite of the excellent safety and efficacy record of EU-approved biosimilars, many physicians still hesitate to prescribe biosimilars. The concept of biosimilarity seems to be difficult to understand and accept as it deviates from the conventional drug development concept [3]. Thus, early position papers of various European and national medical societies failed to recognize the difference. As a result, prescribers were discouraged to use biosimilars in ‘extrapolated’ indications and to switch originators to biosimilars [4]. Since then, more positive position papers [5–7] have been issued. Based on past experience, the understanding of biosimilarity will slowly reach the grass root level of prescribers. During this learning path, many prescribers will suffer from cognitive dissonance [8], i.e. evaluating biosimilars on the basis traditional drug development concept although being informed of biosimilarity. The mighty marketing machineries of pharmaceutical companies that are under threat of biosimilar competition seem to be very skilful in taking advantage of the non-rational aspects of prescription [9–12] in their campaign against biosimilars.
Time is money
The lifespan of a biosimilar that is a copy of a 10+ years old original product is limited. The market of biosimilars is eroded by influx of new products, including new ‘improved’ or ‘biobetter’ versions of the original product. While the benefits of the latter ‘convenience products’, such as the new, more concentrated formulation of original glargin insulin, are often marginal [13], aggressive marketing has managed to convince prescribers to switch patients to the new product that is protected against biosimilar competition. Thus, biosimilar glargin insulins have a negligible market share in most EU countries [14, 15]. In 2016, about half of the epoetin market and two thirds of the filgrastim market were protected by biobetters and subsequently biosimilars were able to take only a modest slice of the total epoetin alfa and filgrastim markets [1]. From the health economical point of view, biosimilars should be adopted to clinical use as soon as possible after marketing authorization in order to get the desired savings.
Interchangeability – suspicions without a smoking gun
Interchangeability is the key factor determining the success of biosimilars whose main market is in chronic treatment. Tendering processes have led to switches between biosimilars and the originator products in several countries without safety problems. Data from controlled and uncontrolled switches have not raised any safety, immunogenicity, or efficacy concerns [16, 17]. Many national regulatory agencies have issued position papers supporting physician-guided switches [18].
O’Brien et al. [19] described the process that led to the prescription of a biosimilar infliximab and later to the switching of the originator infliximab to the biosimilar infliximab in an Irish teaching hospital. This project lasted three years after licensing of the product and was based mainly on clinical studies and position papers. Even then, the hospital pioneered switching in Ireland where negative attitudes against switches are still common [20]. O’Brien et al. [19] predict that prescribers will also require switching studies from other biosimilars. This approach reflects the mistrust in the biosimilar development concept that aims to demonstrate physicochemical, structural, and functional similarity to the extent that the clinical performance will also be similar. Reliance on switch studies generates two problems. First, it will reduce the attractiveness of biosimilar development by increasing costs and narrowing the window of opportunity for biosimilars. Second, it is unlikely that reasonably sized switch studies will give reliable answers, as the potential differences in safety are small and significant problems very rare.
For the success of biosimilars, it will be critical whether clinicians will regard the clinical switching studies conducted thus far as the proof of concept or whether switching studies will always be required between an innovator product and its biosimilars or even between biosimilars of the same innovator product.
First, do not harm is a good principle for payers
Payers and policymakers have noticed the slow uptake of biosimilars and have taken measures to control pricing and prescription. Setting a minimum price reduction compared to the originator and requesting prescription quotas for biosimilars sound logical but may be counterproductive as they will reduce the attractiveness of the local market, especially in small Member States, to biosimilar developers. The market dynamics of biosimilars is different from that in generics market [21, 22]. In the Nordic countries, Denmark and Norway apply national tendering processes that have managed to introduce biosimilars relatively fast and obtained significant price reductions as compared to Finland that requires 30% price reduction and has to wait longer for biosimilars to enter the market. The situation is further complicated by different goals of companies developing biosimilars [1].
Companies developing only biosimilars are ready to price competition whereas for other companies also developing original biologicals, biosimilars are only the plan B. The latter companies do not readily enter price competition and wish to keep regulatory requirements high and competition low.
How about automatic substitution?
Successful use of generics required the introduction of automatic substitution. Several old beliefs of insurmountable problems in copying biological medicines, such as characterization of complex molecules, extrapolation of safety and efficacy, and interchangeability have turned out to be unfounded or greatly overstated. Now, it is time to have a second look at automatic substitution. Irrespective of their attitude to physician-guided interchangeability, position papers of medical societies and anti-biosimilar industry-sponsored publications state categorically that automatic substitution is not appropriate. Automatic substitution at the pharmacy level is currently not possible in most Member States [2, 23]. Larkin et al. [23] listed several prerequisites for automatic substitution, including additional clinical data and designation as an interchangeable biosimilar. Such a requirement will raise the bar for biosimilar development so high that only ‘Big Pharma’ can afford it and, thus, reduces competition. As always with biosimilars, discussion of automatic substitution is often biased by the interests of stakeholders.
What is the difference between physician-guided switching and automatic substitution?
There is a fairly wide consensus in the interchangeability of biosimilars [18]. Automatic substitution is a practical application of interchangeability that will be initiated at the political and administrative level when there are economic constraints and alternative ways to control costs are unpopular or harmful to public health. A prerequisite for automatic substitution is that the pharmacy staff will be able to provide information to patients and caregivers on biosimilars and, if necessary, training in the use of a new administration device. This is not an impossible hurdle for adequately staffed pharmacies. Another concern is traceability when a certain product is prescribed and later another is dispensed in the retail pharmacy. Information sharing between pharmacies, hospitals and prescribers outside hospitals may have to be improved to ensure traceability. This will require special arrangements that may include the development of local IT systems. These measures would be useful in improving traceability and adverse event reporting of biologicals in general. Thus, in most EU Member States, automatic substitution will require careful planning, sometimes changes to the legislation, and some support to pharmacies that will execute the substitution. A general scheme for the automatic substitution would be helpful and could be tailored for local circumstances in EU Member States.
Future of biosimilars
Prescribers and other healthcare professionals, patients, payers, and healthcare administrators are slowly learning the value and nature of biosimilars. Biosimilars will probably be adopted sooner in hospitals where the choice of the medicinal product is not an individual prescriber’s choice and where the budget determines the access to medicines.
The experience from the biosimilar glargin insulin suggests that the adoption of other biosimilars that are prescribed outside hospitals may be slow. Thus, additional measures, carrots and sticks, are needed. It seems likely that an increasing number of EU Member States will consider automatic substitution. Prescribers have to reconsider their role in ensuring the sustainability of the pharmacotherapy in EU – an active player or a bystander.
In the long run, biosimilars will become a standard tool for controlling costs of biologicals produced by biotechnology. The market dynamics of biosimilars is not straightforward and depends on the number of biosimilars coming to the market, as well as attitudes of payers and prescribers. Thus far, the method of restoring healthy competition seems to have been trial and error. In the future, EU Member States will probably adopt more harmonized approach to biosimilar pricing, reimbursement, procurement, prescribing and dispensing policies.
Competing interests: None.
Provenance and peer review: Commissioned; internally peer reviewed.
References
1. QuitilesIMS. The impact of biosimilar competition. May 2017 [homepage on the Internet]. [cited 2018 Mar 11]. Available from: http://www.medicinesforeurope.com/wp-content/uploads/2017/05/IMS-Biosimilar-2017_V9.pdf
2. Moorkens E, Vulto AG, Huys I, Dylst P, Godman B, Keuerleber S, et al. Policies for biosimilar uptake in Europe: an overview. PLoS One. 2017;12(12):e0190147.
3. Woodcock J. Keynote session. DIA/FDA Biosimilars Conference: Guidances, Science, and BsUFA. 12-13 September 2012, Washington DC, USA.
4. Annese V, Avendano-Sola C, Breedveld F, Ekman N, Giezen TJ, Gomollón F, et al. Roundtable on biosimilars with European regulators and medical societies, Brussels, Belgium. Generics and Biosimilars Initiative Journal (GaBI Journal). 2016;5(2):74-83. doi:10.5639/gabij.2016.0502.019
5. Danese S, Fiorino G, Raine T, Ferrante M, Kemp K, Kierkus J, et al. ECCO position statement on the use of biosimilars for inflammatory bowel disease – an update. J Crohns Colitis. 2017;11(1):26-34.
6. Tabernero J, Vyas M, Giuliani R, Arnold D, Cardoso F, Casali PG, et al. Biosimilars: a position paper of the European Society for Medical Oncology, with particular reference to oncology prescribers. ESMO Open. 2016;1(6):e000142.
7. Kay J, Schoels MM, Dörner T, Emery P, Kvien TK, Smolens JS, et al. Consensus-based recommendations for the use of biosimilars to treat rheumatological diseases. Ann Rheum Dis. 2018;77(2):165-74.
8. Phillips S. The evaluation of biosimilars and cognitive dissonance. BHBIA Yearbook. 2015;32.
9. Moorkens E, Jonker-Exler C, Huys I, Declerck P, Simoens S, Vulto AG. Overcoming barriers to the market access of biosimilars in the European Union: the case of biosimilar monoclonal antibodies. Front Pharmacol. 2016;7:193.
10. Avorn J. The psychology of clinical decision making – implications for medication use. N Engl J Med. 2018;378(8):689-91.
11. Albersheim SG, Golan A. The physician’s relationship with the pharmaceutical industry: caveat emptor…buyer beware! Isr Med Assoc J. 2011;13(7):389-93.
12. Lyles A. Biosimilars: patient and physician acceptability is the fifth hurdle to market competition. Generics and Biosimilars Initiative Journal (GaBI Journal). 2015;4(1):6-7. doi:10.5639/gabij.2015.0401.002
13. European Medicines Agency. Assessment report Abrasria. EMA/CHMP/340840/2014. 26 June 2014 [homepage on the Internet]. [cited 2018 Mar 11]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002835/WC500175383.pdf
14. GaBI Online – Generics and Biosimilars Initiative. Biosimilar insulins – reducing the cost of diabetes. [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2018 Mar 11]. Available from: www.gabionline.net/Biosimilars/Research/Biosimilar-insulins-reducing-the-cost-of-diabetes
15. Biogen. Attachment 1: How to maximize savings from biosimilars in Finland [homepage on the Internet]. [cited 2018 Mar 11]. Available from: https://www.eduskunta.fi/FI/vaski/JulkaisuMetatieto/Documents/EDK-2016-AK-86713.pdf
16. Cohen HP, Blauvelt A, Rifkin RM, Danese S, Gokhale SM, Woollet G. Switching reference medicines to biosimilars: a systematic literature review of clinical outcomes. Drugs. 2018. doi:10.1007/s40265-018-0881-y. Epub ahead of print
17. McKinnon RA, Cook M, Liauw W, Marabani M, Marschner IC, Packer NH, et al. Biosimilarity and interchangeability: principles and evidence: a systematic review. BioDrugs. 2018;32(1):27-52.
18. Medicines for Europe. Biosimilar medicines. Positioning statements on physician-led switching for biosimilar medicines Finland [homepage on the Internet]. [cited 2018 Mar 11]. Available from: http://www.medicinesforeurope.com/wp-content/uploads/2017/03/M-Biosimilars-Overview-of-positions-on-physician-led-switching.pdf
19. O’Brien G, Carroll D, Mulcahy M, Walshe V, Courtney G, Byrne S. Biosimilar infliximab introduction into the gastroenterology care pathway in a large acute Irish teaching hospital: a story behind the evidence. Generics and Biosimilars Initiative Journal (GaBI Journal). 2018;7(1):14-21. doi:10.5639/gabij.2018.0701.004
20. O’Callaghan J, Bermingham M, Leonard M, Hallinan F, Morris JM, Moore U, et al. Assessing awareness and attitudes of healthcare professionals on the use of biosimilar medicines: a survey of physicians and pharmacists in Ireland. Regul Toxicol Pharmacol. 2017;88:252-61.
21. Bocquet F, Loubière A, Fusier I, Cordonnier AL, Paubel P. Competition between biosimilars and patented biologics: learning from European and Japanese experience. Pharmacoeconomics. 2016;34:1173-86.
22. Rémuzat C, Dorey J, Cristeau O, Ionescu D, Radière G, Toumi M. Key drivers for market penetration of biosimilars in Europe. J Mark Access Health Policy. 2017;5(1):1272308.
23. Larkin H, Macdonald J, Lumsden R. Pharmacy-mediated substitution of biosimilars – a global survey benchmarking country substitution policies. Generics and Biosimilars Initiative Journal (GaBI Journal). 2017;6(4):157-64. doi:10.5639/gabij.2017.0604.034
|
Author Adjunct Professor Pekka Kurki, MD, PhD, University of Helsinki, 19 Lukupolku, FI-00680 Helsinki, Finland
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2018 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/eu-member-states-have-tools-to-reduce-costs-of-bestseller-biologicals-but-can-they-use-them.html
Potential changes to the FDA approach to biosimilars have a global impact
|
Abstract:
The Opinion article of Niazi urges the US Food and Drug Administration (FDA) to make adjustments to its guidance on biosimilar development. This article comments on some of the proposals from a global perspective, including the global reference product and the biosimilar comparability programme. FDA Commissioner Scott Gottlieb has stated that the biosimilar market suffers from a lack of competition. Therefore, the FDA approach to biosimilars, including many of the issues raised by Niazi will be revisited in the new Biosimilar Action Plan of the FDA.
|
Submitted: 26 July 2018; Revised: 26 July 2018; Accepted: 27 July 2018; Published online first: 30 July 2018
The Opinion article of Adjunct Professor Niazi in this issue of GaBI Journal argues that the US Food and Drug Administration (FDA) could make several adjustments to its guidance in order to facilitate the development of biosimilars [1]. The author points out that the current requirements have led to high costs and long development times which discourage small- and medium-sized enterprises from entering biosimilar development. Indeed, FDA Commissioner Scott Gottlieb has stated that the biosimilar market suffers from a lack of competition [2, 3]. Some of the proposals of the author deserve comments from a global perspective.
Bridging studies and substitution
Acceptance of a foreign-sourced reference product in clinical studies is highly desirable for global development programmes of biosimilars. Repetition of clinical trials in different regulatory regions is unnecessary, expensive and ethically questionable. Most regulatory agencies require ‘bridging studies’ to demonstrate that the foreign-sourced reference product and the corresponding domestic product are highly similar. FDA has the most stringent requirements, including not only analytical comparability but also additional human pharmacokinetic/pharmacodynamic (PK/PD) studies [4].
The author proposes that bridging studies should not be required if the foreign and domestic products have the same composition and have been licenced on the basis of the same documentation. In this case, products sourced from different but ‘highly regulated’ regions should be very similar and safe since they have been used over 10 years under regulatory surveillance. However, if there are significant differences in the regulatory history, there is a theoretical possibility that the two products have ‘drifted apart’ over the years because of different changes to their manufacturing processes. In addition, the waiver of bridging studies may face legal obstacles in some jurisdictions. Nevertheless, the developers should be able to get waivers for at least some bridging studies if they can demonstrate that, based on the regulatory history of the products, differences between the domestic and foreign reference product are highly unlikely. Collaboration and data sharing between the key regulatory agencies would facilitate the acceptance of a global reference product. Global development of biosimilars is in the interest of all countries, including the US. Therefore, FDA should act in a pragmatic way to promote global development of biosimilars.
The author argues that a waiver of bridging studies would not be possible in a study intended to support interchangeable status of a biosimilar product. This recommendation is based on the current FDA draft guideline on the interchangeable biosimilars [5]. Unfortunately, the requirement may create a bottleneck for global development by promoting the use of a US reference product. Furthermore, it would harm the basic concept of biosimilarity by creating two levels of biosimilarity.
Clinical trials
The author makes several proposals to reduce the requirements of PK evaluation. Most of them will not significantly change the burden of PK studies.
The author regards PK studies in healthy volunteers as ethically questionable and proposes PK studies in monkeys.
Single-dose comparative PK studies are recommended by regulators as a simple model with minimal confounding factors in cases where the product can be safely administered to healthy volunteers [6, 7]. The proposal to study disposition kinetics in monkeys is problematic from scientific, ethical and global development points of view. In addition, studies to convincingly demonstrate comparable PK in monkeys are hardly feasible from a practical point of view.
The author promotes the use of in vitro and in vivo non-clinical testing of immunogenicity to justify waivers of clinical immunogenicity studies. While such testing may be useful in the selection of the lead compound for development, the ability of in vitro tests to fully mimic the human immune system is still inadequately documented for regulatory purposes. The issue is not immunogenicity as such. FDA guidance speaks about clinical immunogenicity studies since the ultimate goal of these studies is to look for harmful immunogenicity. For the time being, this is possible only in the context of clinical safety and efficacy studies [8, 9]. Abandoning clinical safety and efficacy studies in a near future would be a strategic mistake considering the mindset of prescribers.
Interchangeability
The ability and willingness to switch between originator products and their biosimilars are the keys to the economic benefits of biosimilars. The author does not comment on the draft interchangeability guideline [5] as it is assumed to be bound to the legal provisions outside the mandate of FDA.
It is assumed by some experts that the US legislation guiding the development of biosimilars is biased because of lobbying by the originator industry [10, 11]. The industry is also active in promoting a very conservative guidance, recently in case of the draft guideline for interchangeability [5]. In general, the current US legislation and guidance may not ensure satisfactory availability biological therapy for patients because they allow anticompetitive behaviour [3].
In the EU, biosimilars are generally regarded as interchangeable under the supervision of the prescriber and in Australia, biosimilars may even be substituted at the pharmacy level [12]. It is unfortunate that the leading regulatory authorities have adopted different policies with regard to interchangeability as it creates confusion and uncertainty among regulators and their stakeholders worldwide.
It would be beneficial for the global market if FDA would clearly separate interchangeability without (automatic) substitution from interchangeability associated with substitution at the pharmacy level and allow prescribers and local regulatory authorities to develop safe methods for switching between a biosimilar and its reference product. After all, FDA approved biosimilars and their reference products, by definition, are highly similar and have no clinically meaningful differences [13]. Tens of clinical switching studies have not raised any significant efficacy or safety signals [14, 15]. The requirement of specific switching studies using the local reference product is a serious blow to the hopes for significant savings for the US healthcare system and may discourage global development of biosimilars.
Education
The author requests FDA to intensify its information on the safety of biosimilars. FDA and other agencies that have licensed biosimilars are in a very unusual situation since the safety of biosimilars is widely and publicly questioned by some parts of the industry. According to the author, this has led to misunderstandings about the safety of biosimilars, ‘integrated into the minds of prescribers and the public by the products’ originator companies’. This situation is difficult to change because only originator companies (Big Pharma) have the resources and channels to reach each individual prescriber.
The problem is not the availability of information on biosimilars. Regulatory agencies, including FDA, have delivered information on the benefit-risk of biosimilar products and their approval process. However, this information is likely to reach only prescribers that have a genuine interest to seek and review the available data, such as opinion leaders who are drafting position papers for their specialties.
The recent consultation on FDA draft guidance on interchangeability clearly demonstrated that the views of physician societies are closely following the opinions of the innovator sector of the industry [16]. This association may be partially due to the lack of understanding/acceptance of the comparability concept, on one hand, and the public health impact of biosimilars, on the other hand. Therefore, FDA is encouraged to engage in frank discussion with medical societies who issue position papers on biosimilars. In Europe, the physician societies originally discouraged biosimilar use [17] but have recently reversed their positions on controversial issues, such as extrapolation of therapeutic indications and interchangeability [18–20]. Such a change may happen also in the US [21].
How to balance innovation and safety with competition and availability – FDA dilemma
The author criticizes the FDA approach to manufacturing, analytical comparisons and clinical development of biosimilars. This discussion is important since FDA has recently published a plan to revise its approach to biosimilars, the Biosimilar Action Plan (BAP) [22]. The goal is to restore the balance between protection of innovation, on one hand, and competition and access to biologicals, on the other hand. Interestingly, FDA will not only take measures to streamline its own processes but also pay attention to the anticompetitive strategies of the manufacturers of the reference products.
The BAP aims to streamline the biosimilar guidance in order to allow more focused development programmes, including critical quality attributes for different classes of biosimilars, development and validation of PD biomarkers tailored to biosimilar development and in silico modelling and simulation to evaluate PK and PD response versus clinical response relationships. In addition, FDA aims to provide additional guidance for biosimilar development. Most importantly, FDA will enhance collaboration with Canada, Europe and Japan aiming on regulatory harmonization as well as addressing the use of foreign reference products and real-world data. Furthermore, FDA will increase its information on biosimilar regulation for its stakeholders, especially healthcare professionals. Thus, many of the points raised in the article of Niazi will be considered.
In designing the regulatory framework for new areas of pharmacotherapy, regulators will initially have to perform a scientific judgement of the benefits and risks while the true risks are not completely known. A conservative approach is justified initially but it should not lead to obstruction of drug development. The same concept can be applied to biosimilars whilst keeping in mind that the uncertainties at the time of licensing are minute as compared to products with a new active substance. In addition, there is a wide experience in real-world use of biosimilars that is a striking contrast to the concerns entertained by the anti-biosimilar lobby and, to a certain extent, to some elements in the regulatory guidance. FDA now has an opportunity to show leadership to the regulation of biosimilars for the benefit of healthcare systems worldwide.
Competing interests: None.
Provenance and peer review: Commissioned; internally peer reviewed.
References
1. Niazi SK. Rationalizing FDA guidance on biosimilars—expediting approvals and acceptance. Generics and Biosimilars Initiative Journal (GaBI Journal). 2018;7(2):84-91. doi: 10.5639/gabij.2018.0702.018
2. Gottlieb S. Capturing the benefits of competition for patients; Speech presented at America’s Health Insurance Plans’ (AHIP) National Health Policy Conference; 2018; Washington, DC.
3. U.S. Food and Drug Administration. Remarks from FDA Commissioner Scott Gottlieb, M.D., as prepared for delivery at the Brookings Institution on the release of the FDA’s Biosimilars Action Plan [homepage on the Internet]. [cited 2018 Jul 26]. Available from:https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm613881.htm
4. U.S. Food and Drug Administration. Scientific considerations in demonstrating biosimilarity to a reference product. Guidance for industry. April 2015 [home page on the Internet]. [cited 2018 Jul 26]. Available from: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM291128.pdf
5. U.S. Food and Drug Administration. Considerations in demonstrating interchangeability with a reference product. Guidance for industry. January 2017 [homepage on the Internet]. [cited 2018 Jul 26]. Available from: https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM537135.pdf
6. U.S. Food and Drug Administration. Clinical pharmacology data to support a demonstration of biosimilarity to a reference product. Guidance for industry. December 2017 [homepage on the Internet]. [cited 2018 Jul 26]. Available from:https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM397017.pdf
7. European Medicines Agency. Similar biological medicinal products containing biotechnology-derived proteins as active substance: non-clinical and clinical issues [homepage on the Internet]. [cited 2018 Jul 26]. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/regulation/general/general_content_001378.jsp&mid=WC0b01ac058002958c
8. U.S. Food and Drug Administration. Guidance for industry. Immunogenicity assessment for therapeutic protein products. August 2014 [homepage on the Internet]. [cited 2018 Jul 26]. Available from:https://www.fda.gov/downloads/drugs/guidances/ucm338856.pdf
9. European Medicines Agency. Immunogenicity assessment of biotechnology-derived therapeutic proteins [homepage on the Internet]. [cited 2018 Jul 26]. Available from: http://www.ema.europa.eu/ema/index.jsp? curl=pages/regulation/general/general_content_001391.jsp&mid=WC0b01ac058002958c
10. Banthia V. Biosimilar regulation: bringing the United States up to speed with other markets. Minn. J.L. Sci. & Tech. 2015;16(2):879-916.
11. Cornes P. The economic pressures for biosimilar drug use in cancer medicine. Target Oncol. 2012;7(Suppl 1):S57-67.
12. Medicines for Europe. Positioning statements on physician-led switching for biosimilar medicines. Updated April 2018 [homepage on the Internet]. [cited 2018 Jul 26]. Available from: https://www.medicinesforeurope.com/wp-content/uploads/2017/03/M-Biosimilars-Overview-of-positions-on-physician-led-switching.pdf
13. U.S. Food and Drug Administration. Guidance for industry on biosimilars: Q & As regarding implementation of the BPCI Act of 2009: background [homepage on the Internet]. [cited 2018 Jul 26]. Available from: https://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm259806.htm
14. Cohen HP, Blauvelt A, Rifkin RM, Danese S, Gokhale SB, Woollett G. Switching reference medicines to biosimilars: a systematic literature review of clinical outcomes. Drugs. 2018;78(4):463-78.
15. McKinnon RA, Cook M, Liauw W, Marabani M, Marschner IC, Packer NH, Prins JB. Biosimilarity and interchangeability: principles and evidence: a systematic review. BioDrugs. 2018;32(1):27-52.
16. LeRay D, Royzman I. Part II: Stakeholder comments on FDA’s interchangeability guidance for biosimilars. Biologics Blog; 2017 [cited 2018 Jul 26]. Available from: https://www.biologicsblog.com/part-ii-stakeholder-comments-on-fdas-interchangeability-guidance-for-biosimilars
17. Annese V, Avendano-Sola C, Breedveld F, Ekman N, Giezen TJ, Gomollón F, et al. Roundtable on biosimilars with European regulators and medical societies, Brussels, Belgium, 12 January 2016. Generics and Biosimilars Initiative J (GaBI Journal). 2016;5(2):74-83. doi:10.5639/gabij.2016.0502.019
18. Danese S, Fiorino G, Raine T, Ferrante M, Kemp K, Kierkus J, et al. ECCO Position statement on the use of biosimilars for inflammatory bowel disease – an update. J Crohns Colitis. 2017;11(1):26-34.
19. Tabernero J, Vyas M, Giuliani R, Arnold D, Cardoso F, Casali PG, et al. Biosimilars: a position paper of the European Society for Medical Oncology, with particular reference to oncology prescribers. ESMO Open. 2016;1(6):e000142.
20. Kay J, Schoels MM, Dörner T, Emery P, Kvien TK, Smolen JS, et al. Consensus-based recommendations for the use of biosimilars to treat rheumatological diseases. Ann Rheum Dis. 2018;77(2):165-74.
21. Bridges SL Jr, White DW, Worthing AB, Gravallese EM, O’Dell JR, Nola K, et al; American College of Rheumatology. The science behind biosimilars: entering a new era of biologic therapy. Arthritis Rheumatol. 2018;70(3):334-44.
22. U.S. Food and Drug Administration. Biosimilar Action Plan: balancing innovation and competition [homepage on the Internet]. [cited 2018 Jul 26]. Available from: https://www.fda.gov/ucm/groups/fdagov-public/@fdagov-drugs-gen/documents/document/ucm613761.pdf
|
Author: Professor Pekka Kurki, MD, PhD, University of Helsinki, 19 Lukupolku, FI-00680 Helsinki, Finland
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2018 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/potential-changes-to-the-fda-approach-to-biosimilars-have-a-global-impact.html
Physicians, Hippocrates and biosimilars: applying ancient principles in a modern society
|
Abstract:
Physicians are pondering the clinical use of biosimilars. A reliance on clinical trials is deeply rooted in the modern healthcare system, whereas comparability and totality of evidence remain unknown concepts. This editorial explores these ideas, with reference to a case study of Italian gastroenterologists.
|
Submitted: 24 October 2016; Revised: 1 November 2016; Accepted: 1 November 2016; Published online first: 7 November 2016
Europe’s healthcare systems are facing ever-increasing costs. Biologicals, a group of biotechnology-derived therapeutic products, are driving the increasing costs of pharmacotherapy. Unless these increasing costs can be contained, the use of new biological medicinal products could be restricted, even in the wealthiest European Union (EU) Member States.
One means of avoiding such price hikes is developing drugs that are equivalent to brand-name products, but without the patent. Copies of biological products are known as biosimilars. In the EU, cheaper copies of some of the best-selling ‘blockbuster’ biologicals, such as etanercept, infliximab (tumour necrosis factor-alpha [TNF-α] inhibitors used to treat autoimmune diseases such as arthritis) and insulin glargine (a long-acting insulin analogue) have been licensed. Biosimilars to other blockbuster biologicals are in the evaluation or development phases [1]. In the EU, biosimilars are developed according to stringent regulatory requirements and those licensed have been shown to be safe and efficacious after over a decade of use.
In principle, biosimilars have the potential to reduce costs and increase access for important medicines. However, the adoption of biosimilars has faced barriers within the healthcare system. With the exception of infliximab, most of the blockbuster biological drugs are used outside of hospitals, within the community. Thus, physicians are in a key position for increasing the use of biosimilars. Illustrating this point, the paper recently prepared by Annese et al. [2] describes use of biosimilars in the Italian healthcare system, including the difficulties doctors face in accepting biosimilars which often bring economic relief but no direct clinical improvements over existing drugs.
The authors also discuss the Italian health insurance system, which provides pharmacotherapy for citizens. In this system, neither physicians nor patients have an incentive to prescribe and use biosimilars. The system is also fragmented and the use of biosimilars varies between regions. Such variation is difficult to explain by medical or scientific reasons. Together, the lack of incentives and lack of coordination between different regions hinder the rational use of biosimilars. Sadly, this situation is not unique to Italy – healthcare systems across the EU have been poorly prepared for the entry of biosimilars.
As in most EU Member States, the substitution of biosimilars at the pharmacy level is not permitted in Italy. Thus, the decision to initiate treatment with a biosimilar or to switch treatment from the originator drug (reference product) to a biosimilar is normally made by hospitals or individual physicians and patients. The Italian Medicines Agency (Agenzia Italiana del Farmaco, AIFA) states in its recent concept paper that biosimilars are safe and efficacious and that a switch from a reference product to its biosimilar copy is possible, but leaves the responsibility for the decision to individual physicians [3]. In contrast, local medical societies, such as Italian Society of Rheumatology, Italian Society of Dermatology, and Italian Group of Inflammatory Bowel Disease, are less positive regarding the use of biosimilars, especially when it comes to blockbuster monoclonals, such as those used to treat autoimmune diseases [4, 5]. Thus, on the whole, Italian physicians, like many of their colleagues in other EU Member States, appear to distrust licensed biosimilars.
The paper of Annese et al. illustrates the dilemma from the point of view of gastroenterologists. On the one hand, it is acknowledged that biosimilars may enable cost savings, improve access to treatment and promote sustainable health care. On the other hand, local medical societies and individual physicians are reluctant to recommend the use of biosimilars.
The willingness of Italian gastroenterologists to accept the biosimilar concept was tested after the launch of the first biosimilar monoclonal antibody, infliximab, in Italy. The sore points for clinicians were the extrapolation of safety and efficacy from another therapeutic indication (rheumatoid arthritis) to inflammatory bowel disease (IBD) and the interchangeability of biosimilars and their reference products. Italian gastroenterologists insist that clinical trials must be performed in IBD, even if comparability has been demonstrated on physicochemical, structural, functional, pharmacokinetic, safety and efficacy levels in rheumatoid arthritis.
However, there is good evidence for the interchangeability of biosimilars. Several small, mainly uncontrolled studies have not raised concerns. The preliminary results of a large controlled Norwegian switch study (NOR-SWITCH) of biosimilar infliximab in its major therapeutic indications, including IBD, indicate no significant differences in safety and efficacy to the reference product [6]. These findings, along with the good safety record of EU biosimilars, suggest that biosimilar and reference products can be switched safely.
These results may not satisfy all gastroenterologists. However, it is extremely difficult to detect small differences in drug activity due to the fluctuation in disease course and pharmacokinetics within an individual patient, as well as variation between production batches of biological products. A demonstration of the lack of such minor differences would require very large studies and make biosimilar development unfeasible. Thus, one has to rely on comparability based on the totality of evidence from physicochemical, structural and functional tests as well as from limited clinical studies. Furthermore, Italian gastroenterologists are reluctant to switch a patient to a biosimilar if their disease is being well controlled with the reference product. This is another blow to biosimilars, because a switch to biosimilar infliximab only makes clinical sense in patients who already respond to infliximab therapy.
According to Annese et al., the patient should be informed that the safety profile of a biosimilar is less well known than that of the reference product. They also refer to legislation that requires physicians to choose the safest alternative product. Taking this advice literally would limit prescriptions of not only biosimilars but also generic (small molecule) drugs.
European regulators maintain the position that biosimilars contain a new version of the active substance of its reference product, just as a manufacturing change will create a new version of a biological product. Thus, the fact that the original infliximab has had more than 30 changes to its manufacturing process without any supporting clinical safety and efficacy studies is difficult to reconcile with the Italian position towards biosimilars, which are developed according to the same principles of comparability.
To support their conservative approach to biosimilars, Annese et al. refer to Hippocrates’ oath cited as ‘first, do not harm’. Some scholars of ethics say that Hippocrates actually said, ‘above all, do not harm more than succour’. The situation becomes even more complex if one considers biosimilars at an interpersonal level. Vaccines provide an extreme example of the problem of the concept ‘first, do not harm’. It has been argued that the benefits to the many outweigh the harms to the few [7]. With biosimilars, the harm would be theoretical and the benefit economical.
The current circumstances, whereby the physician is part of the healthcare system and where responsibility for the sustainability of health care, including the costs of pharmacotherapy, lie on administrative and political levels, which is very far from the circumstances that prevailed during Hippocrates’ time. For biosimilars, prescribers need to balance the theoretical harm to patients with the concrete benefit of improving access to medicines. What would Hippocrates’ advice be today – to do nothing or act?
Annese et al. insist that the choice of the therapy, originator or biosimilar, should be left to the physician and the patient. Because of the slow uptake of biosimilars, this view has already been challenged and even overruled in several countries, including some regions in Italy that have issued administrative orders to prescribe biosimilars [2]. A massive and almost complete switch from the original (reference) infliximab product to its biosimilar copy took place in Denmark in 2015, following the recommendation of an official body [8]. Only 11 adverse effects related to the switch of more than 90% of patients treated with the reference product to a biosimilar infliximab were reported even after a stimulated reporting.
It seems clear that healthcare systems will gradually adopt biosimilars, including the switches from the reference products to biosimilars. The important question is: will physicians be part of the solution or part of the problem?
Competing interests: None.
Provenance and peer review: Commissioned; internally peer reviewed.
References
1. European Medicines Agency. Applications for centralised marketing authorisation [homepage on the Internet]. [cited 2016 Nov 1]. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/regulation/q_and_a/q_and_a_detail_000169.jsp&mid=WC0b01ac0580a45420
2. Annese V, Gabbani T, Annese AL. Biosimilars in Italy: a gastroenterologist’s view Generics and Biosimilars Initiative Journal (GaBI Journal). 2016;5(3):131-3. doi:10.5639/gabij.2016.0503.033
3. Italy’s AIFA outlines challenge of sustainable innovation, proposes important pro-biosimilars change, second concept paper. IHS Markit. 2016 Jun 16.
4. Annese V, Vecchi M. Italian Group for the Study of IBD (IG-IBD). Use of biosimilars in inflammatory bowel disease: statements of the Italian Group for Inflammatory Bowel Disease. Dig Liver Dis. 2014;46(11):963-8.
5. Fiorino G, Girolomoni G, Lapadula G, Orlando A, Danese S, Olivieri I, et al. The use of biosimilars in immune-mediated disease: a joint Italian Society of Rheumatology (SIR), Italian Society of Dermatology (SIDeMaST), and Italian Group of Inflammatory Bowel Disease (IG-IBD) position paper. Autoimmun Rev. 2014;13(7):751-5.
6. Moe L. Nor-Switch: – Safe switch to biosimilar. Dagens Medicin. 2016 Oct 17.
7. Sokol DK. First do no harm revisited. BMJ. 2013;347:f6426.
8. Danish Medicines Agency. Special focus on reported adverse reactions to biological medicines and biosimilars. 2016 [homepage on the Internet]. [cited 2016 Nov 1]. Available from: https://laegemiddelstyrelsen.dk/en/news/2016/~/media/FF5865ABAC6D492AB650739216D65DCB.ashx
|
Author: Adjunct Professor Pekka Kurki, MD, PhD, University of Helsinki, 19 Lukupolku, FI-00680 Helsinki, Finland
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2016 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/physicians-hippocrates-and-biosimilars-applying-ancient-principles-in-a-modern-society.html
Roundtable on biosimilars with European regulators and medical societies, Brussels, Belgium, 12 January 2016
Author byline as per print journal: Vito Annese, MD, PhD; Cristina Avendaño-Solá, MD, PhD; Professor Ferdinand Breedveld, MD; Niklas Ekman, PhD; Thijs J Giezen, MSc, PharmD, PhD; Professor Fernando Gomollón, MD, PhD; Research Professor Pekka Kurki, MD, PhD; Professor Tore Kristian Kvien, MD; Professor Andrea Laslop, MD; Professor Lluís Puig, MD, PhD; Robin Thorpe, PhD, FRCPath; Martina Weise, MD; Elena Wolff-Holz, MD
|
Introduction: Biological drugs are improving therapeutic options for many diseases, but access to these therapies is being held back by costs. Biosimilars offer a lower-cost alternative to the corresponding original therapeutic protein, the reference product, with a comparable quality, safety and efficacy. Despite these apparent advantages, arriving at the best solution for patients will need improved communication between regulators and caregivers.
Methods: Representatives from medical societies (European and national) which had issued or published a position paper on biosimilars met with regulators and related experts to discuss recent revisions of the regulatory assessment principles of biosimilars, review the current positions of societies on biosimilars, and improve dialogue between medical societies and regulators on biologicals, notably biosimilars.
Results: The positions of the European regulators and medical societies are slowly converging. While many questions were answered, productive discussions identified areas of disagreement and uncertainties. The results of these discussions will inform debate and decision-making in the participants’ organizations and home countries.
Conclusions: The picture of biosimilars is becoming clearer, and stakeholders are beginning to understand better the basis of biosimilar development, on one hand, and the reasons for concerns, on the other hand. Different stakeholders – patients, doctors, pharmacists, payers – need different information. Above all, this must be a collaborative exercise.
|
Submitted: 24 January 2016; Revised: 21 April 2016; Accepted: 21 April 2016; Published online first: 4 May 2016
Introduction
Access to biological therapies, despite their clear potential for the treatment of many diseases, is more or less restricted owing to high cost. The problem is likely to continue or even aggravate, as a growing number of biological therapies enter the market. It remains unclear whether healthcare systems will be able to make these therapies widely available. Stakeholders hope that biosimilars will have a significant impact on the sustainability of future pharmacotherapy. Regulators and learned societies, especially medical societies, have prominent roles in guiding the rational use of new medicines, including biosimilars.
European regulators and medical societies were the first to encounter biosimilars, and countries worldwide are looking to Europe for guidance.
The Generics and Biosimilars Initiative (GaBI), with its mission to foster the worldwide efficient use of high quality and safe medicines at an affordable price, organized a roundtable discussion for European regulators and medical societies on biosimilars with the aim of promoting interaction and sharing information in this increasing important area. It is important to respect the expertise and role of each stakeholder in the biosimilar discussion, agree Research Professor and former Chair of the European Medicines Agency’s (EMA) Biosimilar Medicinal Products Working Party (BMWP), Pekka Kurki of the Finnish Medicines Agency, Fimea, and Chair of the Roundtable on Biosimilars, and Dr Robin Thorpe, Deputy Editor-in-Chief of the GaBI Journal, expert of BMWP, formerly Head of Biotherapeutics Group of the UK’s National Institute of Biological Standards and Control and Co-Chair of the Roundtable.
Methods
On 12 January 2016, GaBI held a Roundtable on Biosimilars in Brussels, Belgium, with participation by European regulators and medical societies. The programme offered speaker presentations and parallel discussion groups to provide participants with important and up-to-date information related to many aspects of biosimilars with a focus on the key issues of comparability, extrapolation, interchangeability and substitution, as well as pharmacovigilance. Presentations were in English. The speakers were regulators but not official delegates of any regulatory body.
Results
Differences between regulatory decisions and the recommendations of medical societies
The Roundtable was opened by the Chair, Professor Pekka Kurki, expert of BMWP, with an overview of European Medical Societies’ position papers on biosimilars, see Table 1. Restricting the overview to recent papers that were written in English, he focussed on the concerns and contrasting views contained within these papers with regards to the regulatory decisions. With the growth in biological therapies and the numbers of diseases they treat, there is a steadily growing number of position papers.
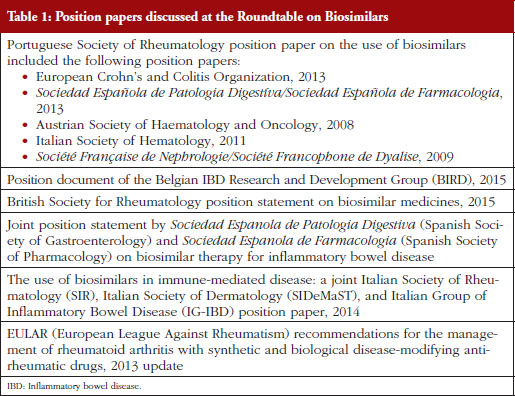
Overall, Professor Kurki noted that these papers were generally in favour of biosimilars, particularly for new patients. But there were mixed opinions on extrapolation, traceability, interchangeability and automatic substitution. Prescribing by brand name was favoured, and there were concerns over immunogenicity.
The biggest problem for physicians, and therefore for medical societies, is that biosimilars can never be exact copies of their reference products. This was a point made throughout the Roundtable in spite of the fact that minor variation of the physicochemical properties of different versions of the same product is an inherent property of all biologicals. Physicians across the board do not find this straightforward to explain to patients. The problem is particularly evident in a naturally relapsing/remitting disease like rheumatoid arthritis (RA). A patient who starts taking a biosimilar and suffers a relapse of symptoms may well blame the symptoms on the biosimilar, and doctors might not always be confident explaining that this is unlikely – given the comparability studies to which each biosimilar will have been subject.
Professor Kurki noted that it is important to recognize that biosimilars have a proven similarity without being identical to the reference product. According to medical societies, even sophisticated comparability testing, in vitro assays and animal studies cannot fully predict the biological and clinical activity of a therapeutic monoclonal antibody.
According to some position papers, extrapolation of indications approved for the originator drug to completely different diseases and age groups that are not based on adequate preclinical, safety and efficacy data (ideally phase I and phase III trials) should not be performed. In their view, extrapolation from rheumatoid arthritis and ankylosing spondylitis studies to Crohn’s disease (CD) and/or ulcerative colitis (UC) cannot be done unless information on mucosal healing, corticosteroid-free remission or immunogenicity and loss of response in CD or UC patients is provided.
The same concerns apply to paediatric patients. Studies specifically looking at outcomes such as growth and development are welcomed by some medical societies.
One concern shared by all the position papers reviewed by Professor Kurki’s team, was that of physician autonomy. It was important for all medical societies that their physicians could make their own therapeutic choices. ‘That is understandable, and we support that. But there are economic realities, and the question is how to apply prescribing autonomy in the best way for the benefit to patients and healthcare systems,’ says Professor Kurki.
Professor Kurki showed a figure illustrating the difference in development philosophies between biosimilars and the reference product, see Figure 1. Two pyramids (representing biosimilars on the left, and originators on the right) represent the marketing authorization documentation. The pyramid representing biosimilars starts at the base with quality documentation (pharmaceutical documentation), followed by an extensive portion dedicated to comparative in vitro studies, analytical, functional and structural testing side-by-side, and then a limited set of clinical trials, and at the top, the risk management plan (RMP). This is clearly different for the development of a new active substance, he notes. While both pyramids share the pharmaceutical documentation, with standards exactly the same for biosimilars as for new biologicals, the originator also has to investigate the pharmacology, the mode of action and the toxicology of the product. For biosimilars, those are already known. Then there is an extensive set of studies for absorption, distribution, metabolism, elimination and pharmacodynamics (PDs). For biosimilars, it is sufficient to demonstrate a comparable exposure after single or repeated administration. In the case of a new biological, every claimed indication needs to be studied, alongside special groups such as children or patients with organ dysfunction. Finally, as with biosimilars, the RMP needs to be in place.
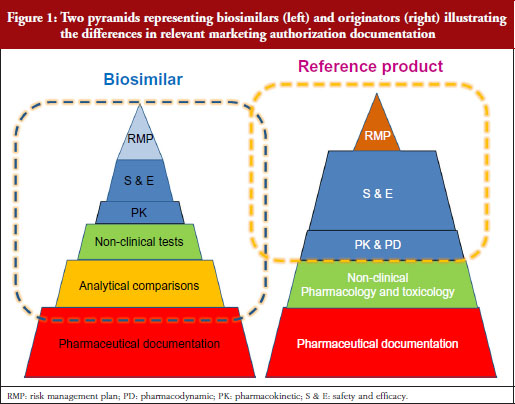
Our problem, suggests Professor Kurki, is that while the regulators look at the analytical and non-clinical testing and the clinical trials as one package (‘totality of evidence’) when deciding what is a biosimilar, clinicians focus on the clinical part only. This would explain, he suggests, the lack of confidence in comparability, while regulators seem more comfortable because they have been carrying out these studies for over two decades for manufacturing changes. This was discussed in more detail by Dr Niklas Ekman, also of Fimea.
Clinical biosimilar safety and efficacy studies look like typical phase III studies, but they are not; they have special features, e.g. looking at population pharmacokinetics (PKs) or PDs markers. Physicians see the active substance of biosimilar as new active substance, whereas regulators see it as a different version of the same active substance.
For specialists, it is difficult to accept that studies performed in one disease can be applied to another disease with different pathogenic features. Regulators, meanwhile, are more focussed on receptor binding and functional tests of the biosimilar, i.e. the mode of action of the active substance.
Manufacturing and characterization of biologicals
Dr Niklas Ekman, a member of EMA’s BMWP, explained how manufacturing process changes are common for all biologicals, both originators and biosimilars. He pointed to earlier studies showing the number of changes made to the manufacturing process of individual products since their approval [1], see Figure 2, and how manufacturing changes impacted on the glycosylation profile and antibody-dependant cell cytotoxicity (ADCC) of biopharmaceuticals – biopharmaceuticals that, from a physician’s point of view, would have been identical [2]. In other words, after a change in manufacturing process, originator biologicals are also not identical to earlier versions of the same originator biological. The comparability concept and its fundamental importance for the maintenance of safety and efficacy have remained unknown to physicians which may explain their reservations to biosimilars.
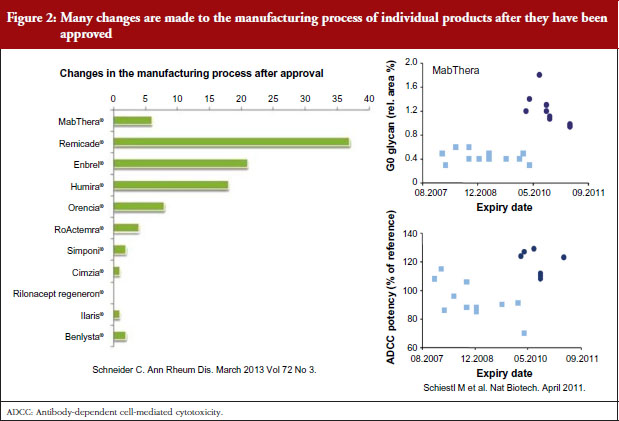
Clinical and non-clinical comparability
Professor Andrea Laslop of the Austrian Medicines Agency and a member of the EMA’s Committee for Medicinal Products for Human Use (CHMP), discussed clinical and non-clinical comparability for biologicals/biosimilars. The non-clinical development is based on the 3Rs: Reduce, Refine and Replace, animal studies as much as possible with in vitro data.
Comparability programmes at the clinical level can and must be strengthened by a number of factors, Professor Laslop urged. Comparability testing must use a homogeneous/sensitive population, a sensitive dose (or two doses), an appropriate model and statistical approach, and must use an accurate definition of the equivalence margin. The primary outcome measures need not be the same as those in the originator’s pivotal clinical trials. Orphan drugs raise unique challenges related to small population sizes. These challenges can be resolved in collaboration with regulatory authorities. Importantly, international dialogue between regulators is needed in order to encourage harmonization of regulatory requirements on a global scale. The final goal, says Professor Laslop, is to provide faster access for patients to affordable biological medicines at a sustainable price.
Immunogenicity
Dr Robin Thorpe, a member of EMA’s BMWP, focussed on the issue of immunogenicity. The European Union was the first to put together a guideline on immunogenicity assessment, he noted, and there is a revised version of this guideline due later in 2016. Immunogenicity issues occur all along the life cycle of a product, and particularly when a new therapeutic protein is developed and used for various clinical indications; when a change in process, formulation, or storage conditions is introduced or – notably given the topic of this roundtable – when a biosimilar product is proposed. Assessment requires an optimal antibody testing strategy alongside validated methodologies and reference standards. A better quality such as decreased immunogenicity does not preclude biosimilarity but needs to be justified as it possibly indicates a difference between products.
Extrapolation
Dr Martina Weise of the Federal Institute for Drugs and Medical Devices in Germany and Vice Chair of EMA’s BMWP discussed the principles of extrapolation of indications. Despite being the most contentious issue of biosimilar development, Dr Weise says extrapolation of indications is the single greatest benefit of biosimilar development.
Noting the data presented by Dr Niklas Ekman, see Figure 2, Dr Weise pointed out that extrapolation of data is already an established scientific and regulatory principle that has been exercised for many years, for example, in the case of changes in manufacturing process of originator biologicals. In such cases, clinical data are not required. In the development of biosimilars, clinical data are typically generated in one indication and, taking into account the overall information gained from the comparability exercise, may then be extrapolated to the other indications.
Dr Weise has recently published a paper on the science of extrapolation [3], with her regulatory colleagues, where the authors say they are not aware of any case of a change in the manufacturing process where more than one clinical study was required to compare two versions of the same product and this was sufficient for all approved indications.
Extrapolation must always be appropriately justified, and, where doubt remains, additional functional or clinical data are required for extrapolation to be granted. Dr Weise reminded delegates that scientific evidence and explanation of the reasons for extrapolation granted by CHMP may be found in the European Public Assessment Reports (EPARs).
Interchangeability
Dr Elena Wolff-Holz of Germany’s Federal Agency for Vaccines and Biomedicines, and a memberof EMA’s BMWP, discussed the interchangeability and substitution of biosimilars. She presented findings from a series of small to medium-sized switching studies involving biologicals and biosimilars, none of which showed any safety/efficacy signals that would justify extensive, longer studies.
For example, a Swedish study that investigated switching between the originator and biosimilar of the growth hormone (somatropin) showed no impact on patients’ growth velocity after switching to the biosimilar, see Figure 3 [4]. When a model was used to compare observed versus predicted growth, the predicted levels lay close to the observed data, showing excellent fit. Similar findings were shown for epoetin alfa-containing biosimilars, biosimilar filgrastim, biosimilar insulin glargine, and biosimilar infliximab. She also emphasized the value of EPARs (European Public Assessment Reports) in which results of biosimilars development programmes (epoetin, filgrastim, insulin glargine, somatropin), which included crossover trials with originators, are presented.
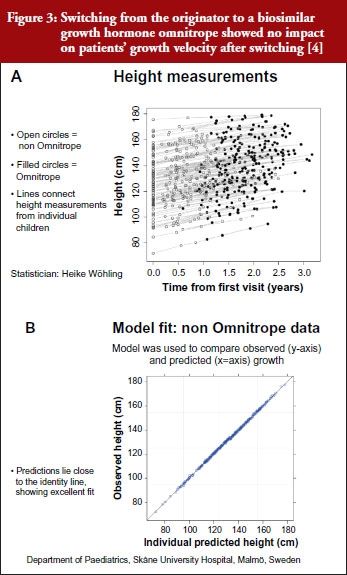
Referring back to the point made by Dr Niklas Ekman, see Figure 2, Dr Wolff-Holz reminded participants of the number of post-marketing changes made to biological drugs, notably monoclonal antibodies, without the need for further clinical studies. The regulators recalled only one case where clinical data were requested. The risk of rare adverse effects is best addressed by the RMP, as with any other medicinal product, she concluded.
Pharmacovigilance
Dr Thijs J Giezen, a hospital pharmacist at the Foundation Pharmacy for Hospitals in Haarlem, The Netherlands, and a member of EMA’s BMWP, discussed the safety assessment and risk management of biosimilars. Safety assessment is of paramount importance for biosimilars, with a particular focus on immunogenicity. Major differences in immunogenicity might question biosimilarity, he noted. As with all drugs, pharmacovigilance for originators and biosimilars is vital, and traceability is of specific importance.
When drawing up a pharmacovigilance plan for a biosimilar, post-marketing studies that not only compare safety profiles but also warn against rare adverse events are in a key position. Additional immunogenicity studies may be considered, perhaps in the context of studies that are already underway, for example, rheumatology registries, or – at a company’s own discretion – initiating new studies.
Summary of discussion about the regulatory presentations
Physicochemical and functional comparability
It was asked whether the quality attributes of a biosimilar and its reference product will be compared in the same way as in the PK bioequivalence studies. It was clarified that, for the key quality attributes, the acceptable range is defined by the analysis of variability between batches of the reference product. For other quality attributes, the acceptable range depends on the type of analytical method. Therefore, statistical analyses are difficult to apply. The products are tested side-by-side to reduce variability. If differences are found, they will be judged by prior knowledge of previous analyses of different versions of proteins in the same class, analysing additional batches, and by using orthogonal methods to look at the same characteristics.
Impact of physicochemical and functional differences on safety and efficacy
Analytical comparability leans on the experience gained from studies of different versions of the active substance after a change of the manufacturing process. These changes are very common because the manufacturing processes need to be optimized, their scale is increased and manufacturing sites changed. Some participants were surprised by the variation between different versions of original biological products that have been accepted without clinical data. It was discussed whether clinical data should be requested more often before accepting a manufacturing change. The regulators responded that there is no evidence from clinical trials performed after licensing, such as expansion of therapeutic indications, that the safety or efficacy of current biotechnology-derived proteins would have changed over time significantly. The explanation is that analytical tests are more sensitive than clinical trials for showing differences.
The demonstration of comparability of monoclonal antibodies is challenging because they have several possible modes of action. Binding to the antigen is necessary for function but Fc-mediated functions may have a role as well. Nevertheless, all functions can be measured by in vitro analytical and functional tests. In the discussion, interpretation of these tests, especially the test for antibody-dependent cell-mediated cytotoxicity (ADCC) was discussed. The audience was concerned about the differences that have been demonstrated after manufacturing changes as well as differences between biosimilars and their reference products. In general, the role of Fc-mediated functions in the therapeutic effect is incompletely known. It was argued that it cannot be excluded that observed ADCC differences (~20%) have an impact on the efficacy or safety. Regulators responded that the differences often disappear when different effector and target cells are used or non-relevant antibodies are present. Sometimes the difference appears only in cells that have Fc-receptors with high affinity genotype. Glycosylation patterns that increase ADCC activity may have a clinical impact. Obinutuzumab is an anti-CD20 antibody that was glyco-engineered in order to enhance the binding to FcγRIIIa. As a result, its ADCC activity against different B-cell lines is 5- to 100-fold higher than that of the ‘wild type’ antibody. This antibody has been shown to be more effective than rituximab in depleting malignant B-cells in chronic lymphocytic leukaemia. Against this background, the small difference in the ADCC between the first biosimilar infliximab and its reference product appears insignificant, especially when considering the applied ADCC test using a target cell line that has been genetically modified to be very sensitive for anti-tumour necrosis factor (anti-TNF) effects.
Interestingly, serious problems after manufacturing changes have been associated with the drug formulation rather than the active substance itself. Pure red cell aplasia (PRCA) has been triggered initially by factors in drug formulation but not with the epoetin alfa itself.
Does comparability mean therapeutic equivalence?
It was asked whether there are examples of seemingly perfect analytical comparability but observed clinical differences at the same time or later. More than 200 cases of PRCA were observed in patients treated with the marketed original epoetin alfa after a manufacturing change. Likewise, decreased efficacy and increased reactogenicity have been observed after manufacturing changes of a few vaccines. So far, such differences have not been observed with biosimilars after licensing. One case of PRCA was detected in a clinical trial with a biosimilar epoetin alfa in development. The development was discontinued. Thus, the experience from the reference product and the extensive comparability exercise will help to identify possible problems already in the development phase of a biosimilar.
Can a biosimilar be better than its reference product?
A product cannot be biosimilar if it has inferior safety or efficacy. However, what if the product is superior? A biosimilar may have an improved quality profile, e.g. purity and immunogenicity. Reduced immunogenicity may lead to slower loss of efficacy and, thus, better adherence to therapy by some patients. Thus, the applicant has to justify the difference with regard to safety and efficacy. Increased efficacy is not possible for a biosimilar since it would make it impossible to refer to the documentation of the reference product which is the basis of the abbreviated development. According to the EU legislation, a ‘biobetter’ must be licensed as a new active substance.
Immunogenicity
It was pointed out that, in the future, there will be several biosimilars for the same reference product. This may lead to multiple switches for the same patient over time. Multiple switches are often said to increase the risks of immunogenicity. Should this scenario be tested before licensing of a biosimilar? Regulators responded that immunogenicity of each biosimilar and its reference product will be compared before licensing. For the time being, data from switching biosimilars and the reference product are reassuring. The current view among European regulators is that, once comparable immunogenicity has been demonstrated against the reference product, there is no need to perform specific switching studies.
Extrapolation
How to select the patient population for a clinical efficacy and safety study when the product is used in different diseases and patient populations using different combinations with other products that may interfere with the performance of the tested active substance was also discussed. It was also asked whether all combinations and diseases and dosing regimens should be tested. Regulators clarified that clinical safety and efficacy studies were preceded by PK and PD studies. The developer should not proceed to large clinical trials if comparability is not demonstrated. The safety and efficacy studies should be done in a clinical model that is representative for other models, i.e. therapeutic indications and populations, and which is sensitive for showing differences. The purpose of the safety and efficacy studies is to complement and confirm the comparability demonstrated at the previous steps of development. This approach requires that the clinical endpoints are sensitive to differences. Thus, the primary clinical endpoints selected for demonstration of comparable efficacy are not necessarily the same as those used in the pivotal clinical trials of the reference product at the time of licensing. For example, overall survival rate and time to progression are generally used in oncology to study a product with a new active substance. These endpoints are time related and usually take rather long time for evaluation. Therefore, a more reasonable and sensitive endpoint, such as overall response rate, may be used. Thus, testing in all therapeutic indications, populations and drug combinations is neither necessary nor feasible.
Disagreements on extrapolation
The concern about extrapolation by clinicians is the use of the same biosimilar or a new innovative product, notably monoclonal antibodies, in different diseases in which the mechanism of action is thought to be different. Infliximab, for example, used in rheumatology is thought to act predominantly through the neutralization of soluble and trans-membrane TNFα, whereas in other conditions such as Crohn’s disease, signalling through membrane-associated forms of TNFα and Fcγ receptors that may trigger apoptosis or ADCC may play a more important role.
Regulators responded by pointing out that the different functions of a therapeutic monoclonal antibody are always investigated by in vitro receptor-binding and cell-based functional assays. These assays are more sensitive than clinical trials. Therefore, regulators feel more comfortable than clinicians with the extrapolation of safety and efficacy between different therapeutic indications.
Clinicians pointed out that clinical experience from less formal, e.g. open label, studies will and have already relieved some concerns about extrapolation.
Clinicians are puzzled by the fact that, in case of the first biosimilar infliximab, Canadian regulators, in contrast to their European colleagues, did not accept the extrapolation of safety and efficacy from RA to inflammatory bowel disease (IBD). Does the fact that all therapeutic indications of the reference product were granted in the EU and later by the US Food and Drug Administration (FDA) mean that the future biosimilar infliximabs, or even etanercepts, will get all therapeutic indications of the reference product automatically? The current regulatory view is that the extrapolation is considered on the basis of the comparability exercise of a given product together with the justification by the applicant. Thus, it is a case-by-case decision.
Regulators’ expectation is that biosimilars approved in the EU will have the same therapeutic indications as the reference product. This is desirable from the pharmacovigilance point of view since a restricted set of therapeutic indications may lead to off-label use. Sometimes, the applicant is not seeking for all therapeutic indications because of patents or because of the lack of suitable, e.g. paediatric, formulation.
Off-target effects and biosimilarity
In general, it is a constant feature of clinical science to observe results that were not expected on the basis of previous knowledge. This is, indeed, almost always the situation after licensing of a product containing a new active substance. It was discussed whether unexpected off-target effects could be observed with biosimilars.
The regulators argued that biologicals, by their nature, have less off-target effects than chemicals. The long experience with the reference products helps to understand the effects of the active substance. A biosimilar will have the same effects, both beneficial and adverse, as the reference product. For biosimilars, the issue is whether new, unexpected off-target effects could be encountered in spite of the extensive comparability exercise. The discussion led to the topic of whether a comparable receptor interaction is sufficient to predict similar functional effects or whether differences in the downstream signalling pathways in target cells could be significantly different after the binding of the biosimilar and the reference product in spite of comparable results in functional cell-based tests, e.g. phagocytosis, apoptosis, ADCC. Regulators maintained that it is essential to separate the effects of the product from the responses of different types of target cells that may respond differently to the same signal. In the end, no agreement was reached on the significance of off-target effects with the use of biosimilars.
A possible off-target effect was mentioned in the context of cancer therapy and bone marrow after treatment with biosimilar filgrastim. Reference was made to the study of Brito et al. (Support Care Cancer. 2016; 24(2):597-603) in early breast cancer receiving (neo)adjuvant docetaxel/doxorubicin/cyclophosphamide therapy and prophylaxis with biosimilar, pegfilgrastim or reference filgrastim. The treatments were administered at different consecutive time periods and data were gathered retrospectively. The rate of febrile neutropenia (FN) per patient and treatment cycle was the same in biosimilar and reference filgrastim groups. The rate of FN and severe neutropenia (ANC < 100 cells/μL) was seen in 50% of patients in the biosimilar group but only in 4% in the reference product group. The authors concluded that ‘No differences in biosimilar effectiveness were detected. The clinical relevance of the profound neutropenia found in the biosimilar cohort needs further attention’. Interestingly, no such difference was found in the multicentre, double-blind, therapeutic equivalence study of biosimilar G-CSF versus the reference product in subjects receiving doxorubicin and docetaxel as combination therapy for breast cancer.
Interchangeability
There is some concern in the rheumatology community about the long delay of full publication of the safety results of the long-term extension of the pivotal safety and efficacy studies of the first biosimilar infliximab, especially the study in ankylosing spondylitis (PLANETAS). During the extension, ankylosing spondylitis patients were switched from the reference product to the biosimilar. The switched patients had a higher rate of adverse events and more withdrawals from the therapy. These results have been reviewed by the EU regulators who did not react to the difference, probably because of the relatively small number of patients at the time of the switch and lack of a plausible explanation. A publication featuring the safety data after the switch is pending.
It was pointed out that neither regulators nor prescribers across the Atlantic have a uniform opinion of the interchangeability. This is partly due to different regulatory frameworks in the two areas and partly due to the interpretation of the theoretical basis and available data.
In the EU, interchangeability is within the mandate of the Member States whereas in the US, interchangeability studies are mandatory by legislation. Interestingly, FDA has not published any guidance on how to study interchangeability. This may reflect the scientific problems related to the switching studies.
Pharmacovigilance
It is evident that the root cause of some adverse effects of biologicals, notably immunogenicity, is in the improper handling and storage of biologicals. It is particularly important to maintain the cold chain. This is becoming a challenge also in Europe when the administration and storage of biological medicines is more and more often taking place at home by the patient or caregiver. Innovative auto injectors and packages may mitigate this problem in the future for biologicals, including biosimilars.
Group discussions (summaries from moderators)
The Roundtable ended with three parallel discussion groups, each of which included representatives from regulatory authorities and from medical societies. Groups were asked to discuss physicians’ attitudes to and concerns surrounding biosimilars – comparability, immunogenicity, extrapolation, interchangeability and substitution, as well as pharmacovigilance. Focus discussion topics included the thought process in preparing position papers, the bottlenecks, e.g. training, and the concerns and challenges faced.
Summary of parallel group discussions
Group 1 Summary
Summarized by Professor Fernando Gomollón, MD, PhD; presented by Professor Ferdinand Breedveld, MD
Group 1 identified a remaining doubt among clinicians, which could be reflected in the question: do in vitro tests really predict the appropriateness of extrapolation? After recognizing that this mere concept can be difficult to accept for clinicians, the general agreement of the group was that if a multiple set of well standardized tests, enough data on exposure in a sensible population and previous clinical data are all considered, extrapolation can be seen as a good concept, a real change of paradigm.
Some issues were raised about safety signals in PLANETAS data. For some people, safety data may require more clarification, although the general opinion was that if EMA had considered the signals as non-significant, they were probably not important.
Registries
There was general agreement among group members on the importance of registries. Ideally these should function on a national scale with a core of data that is easy to share between countries. More work on the definition of these registries is clearly needed.
A real philosophical (or pathophysiological, if preferred) question was also raised. Would a knowledge of the exact mechanism of action of a drug in a given disease make it easier to extrapolate? Perhaps in theory, but with the mechanisms of these diseases being so complex, the general agreement is that the EMA road to extrapolation is adequate in the current state of knowledge.
Good research, poor communication
Some open discussion was undertaken on the low opinion that clinical gastroenterologists have for biosimilars (although it seems rather clear that things are changing and opinions improving). The general agreement was that EMA has done really good scientific work with biosimilars, but not communicated their findings effectively. So, communications should be improved and coordinated, with contributions from EMA, scientific societies and other authorities.
Improving patient care
The group found two concepts that needed emphasizing: 1) biosimilars are not easy to approve in Europe; 2) to date, after approval, the safety record of biosimilars in Europe is really quite good (if not excellent).
Finally, the group agreed that cost is the main drive for biosimilars introduction. This should be seen as an opportunity for better patient care, and that negotiation between payers, authorities, clinicians, pharmacists and patients is the best way to implement change.
Group 2 Summary
Summarized by Cristina Avendaño-Solá, MD, PhD; presented by Vito Annese, MD, PhD
In a group that included four regulators, two rheumatologists, two gastroenterologists, one haematologist and one clinical pharmacologist, there was full agreement on the opportunity that biosimilars provide both in increasing accessibility to biological medicines and in decreasing costs. Those costs can then be diverted to other health spending. Cost benefits are, however, more likely to be related to the arrival of competition, which will drive down the price of the originator drugs. Another possible bonus of biosimilars is seen in preliminary data suggesting that biosimilars could be improvements on originators. They might have less impurities, reduced immunogenicity, or be administered by improved devices.
Switching
One concern shared by the group was how to introduce biosimilars in clinical practice. It is difficult to promote switching between originators and biosimilars in a chronically ill patient who is already taking the originator.
There is still some reluctance about the comparability exercise based on a limited number of parameters and limited clinical data. Recognition of the contribution of data post-authorization and the importance of pharmacovigilance are key.
Concerns were raised about interchangeability. There were doubts related to the absence of data and the potential impact of switching on individual patients. It is complicated to demonstrate interchangeability.
There were also concerns about multiple switching and how to preserve pharmacovigilance and immunogenicity monitoring of each specific product.
Benefits of cost cutting
The group recommended increasing the visibility of the usefulness of the money saved through biosimilars. For example, the agreement of using biosimilars in IBD could go hand-in-hand with actions such as providing extra nurses, support to registers and support for therapeutic drug monitoring (TDM). It is important to recognize the value of TDM to guide switching.
Group members recommended revising how systems of price and reimbursement decisions work at the country level. Involving patients in decision-making will increase their awareness of the benefits of biosimilars.
Group 3 Summary
Summarized and presented by Professor Lluís Puig, MD, PhD
Group 3 focused on monoclonal antibodies for the treatment of immune-mediated inflammatory diseases (IMIDs).
The question was raised whether biosimilars will remove inequity of access to expensive drugs. Group members agreed that access should not depend on price. The UK’s National Institute for Health and Care Excellence (NICE) is working to facilitate entry of biosimilars into the market, but faces many obstacles and concerns among patients and clinicians who are dealing with the unknown.
Switching
The group recognized opposition to switching in patients who are doing well. The only reason for them to switch would be cost, and the group discussed the importance of cost, budgeting and patients’ say. Problems arise around the issue of enforced switching without patients’ consent and full knowledge of safety, or physicians’ choice. The pressure is clearly on the physician. In oncology and haematology there is particularly low acceptance of switching.
The question was raised whether switching trials are needed. Available results show no significant change, but perhaps they are unlikely to do so given their design and power limitations.
In Denmark, there is a 69% discount on Remsima, and authorities enforced wholesale switching. Wholesale switching was similarly promoted in Austria.
NOR-switch is a study funded by the Norwegian Government, aimed to compare the originator infliximab (Remicade) and Celltrion’s biosimilar infliximab (Remsima) as regards disease worsening rates across all indications after one year of treatment. Thirty per cent is the expected worsening rate of Remicade, 15% the non-inferiority margin, and 500 patients are the population enrolled.
Safety
The issue of safety monitoring and the need for registries was discussed. The group raised doubts on quality of monitoring, and asked who will pay for it. In most countries it is unrealistic that governments will pay for monitoring.
In the UK, NICE made a formal requirement that prescribers included new patients treated with biosimilars into registries. There is a need for tracking. There is a need to collect the data regardless of how likely it will be to see a result. There are huge methodological challenges with registries.
Extrapolation
The group looked at real-life data from the Czech Republic showing no difference between originators and their biosimilars. The same was shown for paediatric indications. Regulators do not care so much about the disease in which the trials are being made.
There is a very large difference in perception and acceptance between individual countries. In the Czech Republic, physicians today have no objection to switching and extrapolation based on their results. The situation has changed in 2015, based on education and experience.
Biosimilarity exercise
The group discussed how subjects for clinical trials of biosimilars cannot be found in Western Europe; they have early access to potent therapy and do not progress to levels of activity making them eligible for enrolment. Furthermore, the ethics of a clinical trial that does not provide a clinical advantage was discussed.
There was a concern that PK studies in healthy volunteers may not be representative for all indications in which PK may vary. The regulatory view is that the variability in patients is more dependent on confounding factors than on the active substances.
A request was made for further detail or transparency in preclinical data. An understanding of the way regulatory agencies make their decisions is needed, rather than calling for ever-increasing numbers of clinical trials.
Chair’s observations from the group discussions
It was concluded that biosimilars have the potential to increase patients’ access to biological therapy. Clinicians keep asking for more data and tailored information, especially on the safety and practical conduct of the switches between the biosimilar and its reference product. There is a consensus on the need for a better traceability and surveillance of adverse events of all biologicals. Physicians would like to see data of biosimilars in new or established registries.
Information and transparency are the key issues. It is not only data, as information is available, but only scarce information that is tailored towards different groups of stakeholders. Prescribers, maybe even different specialities, need different information, patients, hospital pharmacists and maybe payers as well. This is one of the take home messages – not only for regulators. Regulators will certainly give a signal to agencies and EMA that the emphasis on information should be even more than it is today.
This information should not only be tailored to the different stakeholders, it also should be focused on certain issues. Information available on several interesting factors can be put together as needed for each stakeholder. One of the issues that has been raised is whether physicians can explain the comparability exercise, especially the physicochemical in vitro biological aspect, and how decision-making is based on those tests.
Prescribers need information on extrapolation, they need to explain why therapeutic indications have been granted without clinical trials. This is another message that delegates at the Roundtable will need to bring back to their organizations and agencies.
The structure–function relationship, what can be said from individual results of analysis, how it can be concluded that a difference in an analytical test is not important, all needs to be explained to patients.
The Chair added one particular target for information, namely extrapolation of safety and efficacy. There are not enough regulators to explain to all stakeholders what extrapolation is, what analytical testing is, and so on. This has to be a collaborative exercise. The information received from London or from Brussels, prepared by multi-disciplinary multi-national teams, is very complicated. This information needs to be tailored according to national healthcare providers and society in general.
Physicians at the meeting were of the opinion that the information on the whole development cascade has helped to put the difficult issues, such as extrapolation and interchangeability, into a clearer context. Yet the limited data on the difficult topics, especially on interchangeability, is still of concern.
The presentation on the physicochemical and structural as well as in vitro functional analyses as the basis for comparability of different versions of both the original and biosimilar products and the long experience of these studies helped clinicians understand the concept of biosimilarity. The fact that the original biological products are not, from a physicochemical point of view, the same as at the time of licensing – because they have been subject to many manufacturing changes over their life cycle – was surprising to some delegates. One delegate even went on to say that it was a shame that physicians had not been aware of the manufacturing process change data shown by Dr Niklas Ekman and others, see Figure 2, which might have made switching to biosimilars less worrying. Any differences in a drug are feared, but it is now clear that physicians have been prescribing non-identical versions of the same drug for years.
Perhaps not surprisingly, the group discussions all agreed that the position of the physician is a difficult one when switching patients from the original product to the biosimilar. Physicians must keep up to date with the latest data in this area, and are personally accountable to their patients for their treatment decisions. On one hand, clinicians do not have the possibility to judge all data that were available for regulators at the time of marketing authorization. On the other hand, positive experience from some members of the groups reduced the level of uncertainty and anxiety.
It is not easy for a physician who has had success with an originator drug to switch to a biosimilar for cost reasons. It may be difficult to persuade a patient to switching to an alternative drug because it is cheaper, rather than because it is better. The health service overall stands to gain through cost savings, not the individual patient. Therefore, switching plans should incorporate some extra values for the patients, increasing their awareness of the benefits of biosimilars.
In at least two discussion groups, it became clear that Czech physicians are relatively unconcerned by switching. This was attributed to a successful education campaign, and to not being under cost pressures. Physicians from other countries often described how they felt they were being put under pressure to make cost savings from which they and their patients would not directly benefit. Perhaps learning about biosimilars and what they are, before being put under pressure to cut costs, would have made switching easier to deal with.
Conflict of interest was mentioned in the discussions. Biosimilarity is an area with high commercial interest. The regulators have extremely stringent rules for conflict of interest. Such rules are not possible in the clinic because it would be very difficult to run clinical trials. Nevertheless, relationships with industry should be somehow managed in order to maintain credibility. This is an issue that both regulators and prescribers need to be very much aware of.
The post-marketing follow-up is another area where physicians and regulators have common interests, especially how to make the most of registries. Current registries have been useful but there have been clear drawbacks; they are not available in every country, the ones that exist are useful for certain purposes but they are not compatible with each other, and it can be difficult to get information by pooling the data from different registries.
The national agencies should consider ways to contribute to registries. There are economic issues; who will fund the registries, how will the people who maintain it be reimbursed? This is also a political issue, since people are sensitive with their information/personal data and hence, permission from the patient is needed to use the data. This is an area where collaboration is required, including a strong signal from clinicians and regulators that these data are important for health care and for individual patients.
Traceability was discussed in the context of having several biosimilars, price competition and tendering processes. This situation may lead to multiple switches that should be documented. TDM was considered slightly outside the typical regulatory scope. There is some information in the summary of product characteristics if the company has been able to provide the necessary information. However, usually this is not the case and TDM is more for academics and clinicians who develop these systems.
Costs were not included in the presentations of this meeting although there is no other incentive to use biosimilars than lower price/costs. Physicians may have to change their role in the biosimilar discussion. The positive consequences of the price competition that is triggered by biosimilars needs to be understood. Roundtable Chair Professor Pekka Kurki hoped that delegates did not mind this kind of remark: ‘Economics are there and times will not improve, it will be harder in the future,’ he said. Instead of maintaining a very conservative attitude, there is another option to become active and try to get the best out of this situation, he said. ‘Think what you can do to induce cost savings with your prescription behaviour. There are examples, from the Czech Republic and the UK, as to how biosimilars can help save money that can be used for other purposes.’
Conclusions of the roundtable meeting
The Roundtable Chair concluded that the pleasant and constructive atmosphere of the meeting supported fruitful discussions, and testified for the importance of dialogue between regulators and physicians. Dialogue increases the mutual trust that is needed when new products and concepts are introduced to health care. The story of biosimilars is not yet at its end, this meeting was an interim analysis. Stakeholders need to be vigilant as the story unfolds.
It appears that the information on biosimilars has not been sufficient to satisfy the needs of prescribers. Physicians were interested in the way physicochemical, structural analyses and in vitro functional tests are used to demonstrate comparability and in the definition of acceptable differences. EPARs contain valuable information on biosimilars. However, their value for clinicians would increase if the crucial decisions such as extrapolation would be better justified. The European regulatory network, EMA and national regulatory agencies, need to find solutions to fill the obvious information gap.
Most of the position papers of medical societies were quite conservative and some contained requirements that would make the development of biosimilars unfeasible. It is evident that prescribers and regulators have different understanding of the biosimilar concept. The situation is changing since more information has become available and since experience from countries that have introduced biosimilars in massive scale, including switches, has been reassuring.
As a consequence, biosimilars are seen more often as an opportunity than a threat. A new situation is emerging in which regulators and prescribers can collaborate in planning managed switches and in tailoring information to various stakeholders, patients, pharmacists, payers. Pharmacovigilance was recognized as an important field of collaboration. Adverse effect reporting of biologicals, including the batch numbers, should be intensified. Collaboration between and within healthcare centres and hospitals as well as pharmacies is necessary to ensure traceability and early detection of rare adverse effects. Regulatory authorities may be able to promote the use of registries in monitoring the use of biosimilars.
Prescribers are in an uncomfortable situation when planning switches in individual patients who will not get immediate benefit and who may have concerns in using biosimilars instead of the original product. Payers and hospital administration should consider granting some incentives to healthcare units that will introduce biosimilars to their patients, e.g. the possibility to use the saved money to improve patient care by introducing new therapies.
Closing the meeting, Co-Chair Robin Thorpe explained that an event like this could only be the first step to reaching a consensus. The strength of such a Roundtable format allowed stakeholders from different and sometimes opposing camps – physicians (rheumatologists, gastroenterologists, dermatologists, haematologists, oncologists), pharmacists and regulators – to discuss their principles and concerns openly. Any conclusions from the event can only reflect what was agreed at the meeting, and what was not agreed.
Speaker Faculty, Moderators and Participants
Speakers
Niklas Ekman, PhD, Finland
Thijs J Giezen, MSc, PharmD, PhD, The Netherlands
Research Professor Pekka Kurki, MD, PhD, Finland (Chair)
Professor Andrea Laslop, MD, Austria
Robin Thorpe, PhD, FRCPath, UK (Co-Chair)
Martina Weise, MD, Germany
Elena Wolff-Holz, MD, Germany
Moderators and Co-moderators
Vito Annese, MD, PhD, Italy
Cristina Avendaño-Solá, MD, PhD, Spain
Professor Ferdinand Breedveld, MD, The Netherlands
Professor Fernando Gomollón, MD, PhD, Spain
Professor Tore Kristian Kvien, MD, Norway
Professor Lluís Puig, MD, PhD, Spain
Participants
Miguel Angel Abad Hernandez, MD, Spain, Spanish Society of Rheumatology (SER)
Vito Annese, MD, PhD, Italy, Italian Group for the Study of IBD (IG-IBD)
Professor Federico Argüelles-Arias, MD, PhD, Spain, Spanish Society of Gastroenterology (SEPD)
Cristina Avendaño-Solá, MD, PhD, Spain, Spanish Society of Clinical Pharmacology (SEFC)
Professor Jürgen Braun, MD, Germany, German Society for Rheumatology (DGRh)
Professor Ferdinand Breedveld, MD, The Netherlands, European League Against Rheumatism (EULAR)
Professor Antonio Costanzo, MD, Italy, Italian Society of Dermatology (SIDeMaST)
Professor Maurizio Cutolo, MD, Italy, European League Against Rheumatism (EULAR)
Assistant Professor Marc Ferrante, MD, PhD, Belgium, European Crohn’s and Colitis Organisation (ECCO)
Professor Fernando Gomollón, MD, PhD, Spain, European Crohn’s and Colitis Organisation (ECCO)
Professor Dr Richard Greil, MD, Austria, Austrian Society of Hematology and Medical Oncology (OeGHO)
Barney Hawthorne, DM, UK, British Society of Gastroenterology (BSG)
Ana Hidalgo-Simon, MD, PhD, UK, European Medicines Agency (EMA)
Professor Tore Kristian Kvien, MD, Norway, European League Against Rheumatism (EULAR)
Professor Milan Lukáš, MD, PhD, Czech Republic, Czech Society of Gastroenterology (CSG)
Professor Alexander MacGregor, MD, PhD, UK, British Society for Rheumatology (BSR)
Professor Massimo Massaia, MD, Italy, Italian Society of Experimental Hematology (IESS)
Associate Professor Dan Nordström, MD, PhD, Finland, Finnish Society of Rheumatology (FSR)
Marieke Pereboom, PharmD, The Netherlands
Bea Perks, PhD, UK
Professor Roberto Perricone, MD, Italy, Italian Society for Rheumatology (SIR)
Laura Pirilä, MD, Finland, Finnish Society of Rheumatology (FSR)
Professor Lluís Puig, MD, PhD, Spain, European Academy of Dermatology and Venereology (EADV)
Riccardo Saccardi, MD, Italy, Italian Group for Bone Marrow Transplantation (GITMO)
Professor Maria-Jesús Sanz Ferrando, PhD, PharmD, Spain, Spanish Society of Pharmacology (SEF)
Lasia Tang, BSc, MBA, Belgium
Apologies
Gonzalo Calvo, MD, PhD, Spain, European Association of Clinical Pharmacology and Therapeutics (EACPT)
Professor Marco Matucci Cerinic, MD, PhD, FRCP, honfbsr, Italy, Italian Society for Rheumatology (SIR)
Professor Silvio Danese, MD, PhD, Italy, European Crohn’s and Colitis Organisation (ECCO)
Professor João Eurico Cortez Cabral da Fonseca, MD, PhD, Portugal, Portuguese Society of Rheumatology (PSR)
Professor Maurizio Vecchi, MD, Italy, Italian Group for the Study of IBD (IG-IBD)
Acknowledgement
The Generics and Biosimilars Initiative (GaBI) wishes to thank Research Professor Pekka Kurki for his strong support through the offering of advice and information during the preparation of this Roundtable meeting.
The authors would like to acknowledge the help of all the roundtable speaker faculty and participants, each of whom contributed to the success of the meeting and the content of this report as well as the support of the moderators: Dr Vito Annese, Dr Cristina Avendaño-Solá, Professor Ferdinand Breedveld, Professor Fernando Gomollón, Professor Tore Kristian Kvien and Professor Lluís Puig, in facilitating meaningful discussion during the parallel group discussions, and presented the discussion findings at the meeting.
The authors wish to thank Dr Bea Perks, GaBI Journal Editor, in preparing this meeting report manuscript and providing English editing support on the group summaries and for finalizing this manuscript.
Editor’s comment
The PLANETAS and PLANETRA extension studies including full safety data have been published online in Annals of Rheumatic Diseases after the meeting of Roundtable on biosimilars with European regulators and medical societies: Park W, et al. Efficacy and safety of switching from reference infliximab to CT-P13 compared with maintenance of CT-P13 in ankylosing spondylitis: 102-week data from the PLANETAS extension study. Ann Rheum Dis. 2016;0:1-9. doi:10.1136/annrheumdis-2015-208783
Yoo DH, et al. Efficacy and safety of CT-P13 (biosimilar infliximab) in patients with rheumatoid arthritis: comparison between switching from reference infliximab to CT-P13 and continuing CT-P13 in the PLANETRA extension study. Ann Rheum Dis 2016;0:1-9. doi:10.1136/annrheumdis-2015-208786
Competing interests: The Roundtable meeting was sponsored by an unrestricted educational grant to GaBI from Hospira UK Ltd.
Provenance and peer review: Not commissioned; internally peer reviewed.
Authors
Vito Annese, MD, PhD
Cristina Avendaño-Solá, MD, PhD
Professor Ferdinand Breedveld, MD
Niklas Ekman, PhD
Thijs J Giezen, MSc, PharmD, PhD
Professor Fernando Gomollón, MD, PhD
Research Professor Pekka Kurki, MD, PhD
Professor Tore Kristian Kvien, MD
Professor Andrea Laslop, MD
Professor Lluís Puig, MD, PhD
Robin Thorpe, PhD, FRCPath
Martina Weise, MD
Elena Wolff-Holz, MD
References
1. Schneider CK. Biosimilars in rheumatology: the wind of change. Ann Rheum Dis. 2013 Mar;72(3):315-8.
2. Schiestl M, Stangler T, Torella C, Cepeljnik T, Toll H, Grau R. Acceptable changes in quality attributes of glycosylated biopharmaceuticals. Nat Biotechnol. 2011;29(4):310-2.
3. Weise M, et al. Biosimilars: the science of extrapolation. Blood. 2014;124(22):3191-6.
4. Flodmark CE, et al. Switching from originator to biosimilar human growth hormone using dialogue teamwork: single-center experience from Sweden. Biol Ther. 2013;3:35-43.
5. GaBI Online – Generics and Biosimilars Initiative. Norwegian study may be slowing adoption of biosimilar infliximab [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2016 Apr 21]. Available from: www.gabionline.net/Biosimilars/News/Norwegian-study-may-be-slowing-adoption-of-biosimilar-infliximab
|
Author for correspondence: Research Professor Pekka Kurki, MD, PhD, Finnish Medicines Agency, PO Box 55, FI-00034 Fimea, Finland
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2016 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/roundtable-on-biosimilars-with-european-regulators-and-medical-societies-brussels-belgium-12-january-2016.html
Biosimilars for prescribers
|
Abstract:
Biosimilars are copies of original biological medicines. Biosimilarity is a new concept in drug development. Physicians prescribing biologicals need more neutral information on the quality, safety and efficacy of biosimilars.
|
Submitted: 27 November 2014; Revised: 15 December 2014; Accepted: 18 December 2014; Published online first: 19 December 2014
Introduction
The European Union (EU) was the first highly regulated area to create a legal and regulatory framework for copies of original innovative biological medicines, similar biological medicinal products (biosimilars). There are currently 19 biosimilars with a valid marketing authorization in the EU. These products represent different levels of structural complexity and are used in several therapeutic areas. In contrast to the pharmaceutical community, where biosimilars have been intensively debated, the interest among physicians has been very modest.
Do physicians understand the concept of biosimilarity?
Dolinar and Reilly [1] published a survey of 470 prescribers in France, Germany, Italy, Spain and UK. Respondents were all specialists who prescribe biologicals, including nephrologists, rheumatologists, dermatologists, neurologists, endocrinologists and oncologists. Only 22% of the specialists claimed to be well informed about biosimilars, even if most responders were affiliated with a hospital or an academic medical centre. Only 19% used the European public assessment reports (EPARs) as a regular source of information. Instead, 47% of responders had acquired their information during seminars and conferences. Thus, regulators and prescribers seem to be disconnected.
An interview-based survey among Finnish specialists [2] reported that several specialists felt that the interchangeability of biosimilars is difficult to evaluate because biosimilars are ‘similar but not the same’. In addition, quality and immunogenicity issues were also of concern to some interviewees. A fraction of specialists had problems in understanding extrapolation of indications, i.e. extrapolation of therapeutic similarity tested in one indication to other indications of the reference medicinal product. In general, specialists requested additional information on biosimilars to decrease the prevailing uncertainty.
Aapro [3] described the concerns of oncologists. Their main concerns come down to the slogans ‘Similar but not the same’ and ‘The product is the process’, i.e. small differences could lead to differences in safety, efficacy and immunogenicity.
There are major differences in the uptake of biosimilars in the EU Member States [4]. These differences may be partly explained by the level of information available to prescribers.
Educating prescribers
The main point in many articles dealing with biosimilars has been that biosimilars are not generics and, therefore, the extrapolation and interchangeability are questioned [5, 6]. Another factor that has muddled the biosimilar waters is the use of the term ‘biosimilar’ for any copy of the biological product including those that have been licensed outside the highly regulated regions [6].
Basics
It is essential that the prescriber can distinguish EU biosimilars from ‘biosimilars’ in other regions [7]. The definition of the biosimilar in the Committee for Medicinal Products for Human Use ‘Guideline on similar biological medicinal products’ [8] is very helpful as a starting point for discussion of biosimilars.
‘A biosimilar is a biological medicinal product that contains a version of the active substance of an already authorized original biological medicinal product (reference medicinal product) in the EEA [European Economic Area]. Similarity to the reference medicinal product in terms of quality characteristics, biological activity, safety and efficacy needs to be established based on a comprehensive comparability exercise’.
This definition contains at least two very important messages. First, the biosimilar contains a new version of the active substance of the reference product. The definition helps to explain that a biosimilar is a very close copy as compared to biobetters, unrelated products targeting the same receptor, line extensions, etc. The second point is that the comparability exercise is the way to demonstrate that different versions of a biological substance have similar efficacy and safety.
Product is the process
Clinicians tend to focus on clinical data only. However, biosimilars should be judged on the basis of the totality of evidence [9]. The development of a biosimilar is based on an extensive comparability exercise where the biosimilar is compared to its reference by physicochemical and structural analyses as well as by in vitro functional tests [10]. Human pharmacokinetic studies will ensure a comparable exposure and a confirmatory clinical trial in at least one therapeutic indication will be conducted. The slogan ‘The product is the process’ cannot be used as an argument against the development of biosimilars. The current biosimilars have proven that a biological product can be copied.
Similar but not the same – comparability
There is extensive experience in comparability studies that control the safety and efficacy of biologicals after manufacturing changes. Current methods to analyse physicochemical and structural differences are extremely sensitive. Analysis of manufacturing batches of the originator (reference) products has revealed differences after a change in the manufacturing process between the pre- and post-change batches [11]. In these cases, no clinical studies were performed. These differences were similar to those that have raised a lot of concerns when observed between a biosimilar and its reference product. Thus, the slogan ‘Similar but not the same’ applies to originator products at the time of licensing and today!
Extrapolation and mechanism of action
Several learned societies have published recommendations and position papers advising prescribers to refrain from using biosimilars in therapeutic indications that have not been studied in clinical trials [12]. The fear of extrapolation is surprising considering the experience from the manufacturing changes of the reference products and line extensions of the reference products [12]. For biosimilars, the extrapolation has to be justified for each therapeutic indication considering the mode of action of the active substance and the characteristics of the target patient populations. If the mechanism of action of the active substance is different in different therapeutic indications, additional data need to be delivered. An illustrative example is the extrapolation of the indications in the case of biosimilar infliximab [13] where additional data were requested to support extrapolation. No problems have been encountered with the extrapolated therapeutic indications of the current biosimilars in the EU.
No formal switch studies – so what?
For the time being, there is no EU regulatory guidance on interchangeability. Nevertheless, there are both theoretical and clinical arguments to support interchangeability of the EU biosimilars. For many reasons, clinical interchangeability studies may not be feasible [14, 15].
In terms of efficacy, it is unlikely that products containing different versions of the same active substance and being comparable at the population level would act differently in an individual patient. Theoretically, differences might occur if the formulations of the biosimilar and the reference product would be very different causing inter-patient variability. This possibility can be clarified by reviewing EPARs of the biosimilars available on the EMA (European Medicines Agency) website.
Currently, the main concern of switching patients from a reference product to its biosimilar is immunogenicity. There is no theoretical basis or clinical evidence suggesting that a switch itself would cause immunogenicity. The known examples of switch-related immunogenicity have occurred after a manufacturing process change of an innovator product resulting in an inferior version of the product.
An inferior immunogenicity profile of a biosimilar cannot be completely ruled out but it is unlikely for two reasons. First, the anti-drug antibody (B-cell) responses of biosimilars are always investigated before marketing authorization [16]. An inferior immunogenicity profile is not compatible with biosimilarity. Second, the active substance of a biosimilar has the same amino acid sequence as the reference product and, thus, shares the linear T-cell epitopes. A strong immune response would require a new T-cell epitope. In addition, the levels of immunogenic impurities and aggregates are tightly controlled. Finally, the knowledge of serious immunological complications of the innovator product, such as pure red cell aplasia triggered by epoetin alfa, will help the biosimilars developer to be prepared for the potential problem and to prevent the entry of an inferior product to the market [17].
Ebbers et al. [18] looked for evidence of switch-related adverse effects from three sources: the EudraVigilance database for serious adverse effects of biosimilars; prospective switch studies of two versions of the same product, including biosimilars; and retrospective studies that involved sequential use of biologicals. They found no signal of switch-related adverse effects. This is reassuring for a prescriber who will consider a switch from the reference to its biosimilar version.
Carrots and sticks to prescribers
Switching to a biosimilar seems not to offer any benefit for an individual patient or prescriber. The motivation has to come from a wider understanding of the role of biosimilars to support sustainable pharmacotherapy. Many prescribers are already facing rationing of biological therapies because of their high costs [3]. Considering the increasing role of biologicals in pharmacotherapy, this problem will escalate rapidly. Thus, a prescriber must weigh the inconvenience and potential risk of switching, on one hand, and patient access to biologicals, on the other. Prescribers could be given an easier access to new medicines provided that they use biosimilars.
The relationship of prescribers to biosimilars is somewhat similar to attitudes towards generics in the past. Experience with generics suggests that the payers will not tolerate a very slow uptake of biosimilars. France has already taken the first step by introducing the possibility of substituting reference products for their biosimilars in first-time users of biologicals [19].
Conclusions
Currently, many physicians hesitate to use biosimilars and would like to have more information. It is important that regulators in the EU Member States distribute information that is already available. Otherwise, prescribers are left with information that is influenced by commercial interests. The problems encountered in the EU are probably shared by other regions as well.
The key messages that need to be conveyed to prescribers are:
- A biological product can be copied by an extensive comparability programme and reverse engineering of the manufacturing process of the biosimilar
- The current biosimilars in the EU have proven to be of high quality and as efficacious and safe as their reference products
- There are always some differences between the reference and biosimilar products. However, the same type of differences is seen after manufacturing changes of the reference products between the pre- and post-change versions
- Extrapolation of therapeutic indications is based on scientifically valid criteria. Thus far, no problems have been encountered with the ‘extrapolated’ indications of biosimilars
- Available data suggest that the current EU biosimilars are interchangeable with their reference products
For patients
Most therapeutic proteins are produced by a biotechnological manufacturing process, i.e. by living cells. Products that are derived from living cells are always heterogeneous. Therefore, there is some variation between production batches, especially if the manufacturing process is changed. The manufacturers have to do comparability studies to demonstrate that the safety and efficacy of the product has not changed after the change in the manufacturing process. Biosimilars are new versions of original biological medicines. Biosimilars are shown to be comparable to the original medicine by extensive comparability studies. This approach to drug development is not well known to physicians who prescribe biological medicines. Therefore, physicians have been reluctant to prescribe biosimilars. The purpose of this manuscript is to summarize the information that is essential for the prescriber to become confident in the quality, safety and efficacy of biosimilars.
Biosimilars have been shown to reduce the costs of biologicals and, in this way, to improve patients’ access to important medicines.
Competing interests: None.
Provenance and peer review: Commissioned; externally peer reviewed.
References
1. Dolinar R, Reilly M. Biosimilars naming, label transparency and authority of choice – survey findings among European physicians. Generics and Biosimilars Initiative Journal (GaBI Journal). 2014 3;3(2):58-62. doi:10.5639/gabij.2014.0302.018
2. Merikoski M, Finnish Medicines Agency, personal communication, 2014.
3. Aapro MS. What do prescribers think of biosimilars? Targ Oncol. 2012;7 Suppl 1:S51-5.
4. GaBI Online – Generics and Biosimilars Initiative. Biosimilars use in Europe [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2014 Dec 15]. Available from: www.gabionline.net/Reports/Biosimilars-use-in-Europe.
5. Genazzani A, Biggio G, Caputi AP, Del Tacca M, et al. Biosimilar drugs: concerns and opportunities. BioDrugs. 2007;21(6):351-6.
6. Qureshi Z, Magwood JS, Singh S, Bennett CL. Rituximab biosimilars – equivalence and reciprocity. Biosimilars. 2013(3):19-25.
7. Weise M, Bielsky MC, De Smet K, Ehmann F, et al. Biosimilars – why terminology matters. Nat Biotechnol. 2011;29(8):690-3.
8. European Medicines Agency. Guideline on similar biological medicinal products. CHMP/437/04. 30 October 2005 [homepage on the Internet]. 2005 Nov 11 [cited 2014 Dec 15]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2014/10/WC500176768.pdf
9. Weise M, Bielsky MC, De Smet K, Ehmann F, Ekman N, Giezen TJ, et al. Biosimilars: what clinicians should know. Blood. 2012;120(26):5111-7.
10. McCamish M, Woollett G. The continuum of comparability extends to biosimilarity: how much is enough and what clinical data are necessary? Clin Pharmacol Ther. 2013;93(4):315-7.1
11. Schiestl M, Stangler T, Torella C, epeljnik T, et al. Acceptable changes in quality attributes of glycosylated biopharmaceuticals. Nat Biotechnol. 2011;29(4):310-2.
12. Weise M, Kurki P, Wolff-Holz E, Bielsky MC, Schneider CK. Biosimilars: the science of extrapolation. Blood. 2014;124(22):3191-6.
13. European Medicines Agency. Remsima assessment report. EMA/CHMP/589317/2013. 27 June 2013 [homepage on the Internet]. 2013 Sep 30 [cited 2014 Dec 15]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002576/WC500151486.pdf
14. Endrenyi L, Chang C, Chow SC, Tothfalusi L. On the interchangeability of biological drug products. Stat Med. 2013;32:434-41.
15. Ebbers H, Chamberlain P. Interchageability. An insurmountable fifth hurdle? Generics and Biosimilars Initiative Journal (GaBI Journal). 2014;3(2):88-93. doi:10.5639/gabij.2014.0302.022
16. European Medicines Agency. Guideline on immunogenicity assessment of biotechnology-derived therapeutic proteins. EMEA/CHMP/BMWP/14327/2006. 13 December 2007 [homepage on the Internet]. 2008 Jan 10 [cited 2014 Dec 15]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003946.pdf
17. Haag-Weber M, Eckhardt KU, Hörl WH, Roger SD, et al. Safety, immunogenicity and efficacy of subcutaneous biosimilar epoetin-α (HX575) in non-dialysis patients with renal anemia: a multi-center, randomized, double-blind study. Clin Nephrol. 2012;77(1):8-17.
18. Ebbers HC, Muenzenberg M, Schellekens H. The safety of switching between therapeutic proteins. Expert Opin Biol Ther. 2012;12(11):1473-85.
19. GaBI Online – Generics and Biosimilars Initiative. France to allow biosimilars substitution [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2014 Dec 15]. Available from: www.gabionline.net/Policies-Legislation/France-to-allow-biosimilars-substitution
|
Author: Pekka Kurki, MD, PhD, Research Professor, Finnish Medicines Agency, PO Box 55, FI-00034 Fimea, Finland
|
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2015 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/biosimilars-for-prescribers.html
Copyright ©2025 GaBI Journal unless otherwise noted.
Generics and Biosimilars Initiative (GaBI)
Tel: +32 474989572 | Fax: +32 14 583 048
EU Member States have tools to reduce costs of bestseller biologicals but can they use them?
Abstract:
Major cost savings are achievable in pharmacotherapy in the European Union since biosimilars to most best-selling biological medicinal products have been licensed. Unfortunately, the window of opportunity may be missed since neither national pricing, reimbursement and procurement systems nor prescribers are well prepared for biosimilars’ entry to the market.
Submitted: 9 March 2018; Revised: 11 March 2018; Accepted: 12 March 2018; Published online first: 23 March 2018
Introduction
Biosimilars to most blockbuster biologicals have now been licensed in the European Union (EU). The key biologicals have estimated sales of Euros 40 billion in 2016–2020 in the main European markets [1]. Thus, the healthcare systems in the EU will soon get a relief provided by great savings and a better access to important medicines – or maybe not?
The problem is that EU Member States do not have a common master plan or shared idea as how to collect the reward for having biosimilars approved. Decisions for interchangeability, price, reimbursement, procurement and instructions to prescribers are made separately in each Member State [2]. The final decisions to use biosimilars are usually made by individual hospitals and prescribers. By each step, different decisions are made. Because of this highly complicated situation, biosimilars have had a very modest and variable success in penetrating the markets dominated by originator products. At the moment, prescribers are the main gatekeepers for biosimilars into the health care.
Prescribers suffer from lack of knowledge and motivation
In spite of the excellent safety and efficacy record of EU-approved biosimilars, many physicians still hesitate to prescribe biosimilars. The concept of biosimilarity seems to be difficult to understand and accept as it deviates from the conventional drug development concept [3]. Thus, early position papers of various European and national medical societies failed to recognize the difference. As a result, prescribers were discouraged to use biosimilars in ‘extrapolated’ indications and to switch originators to biosimilars [4]. Since then, more positive position papers [5–7] have been issued. Based on past experience, the understanding of biosimilarity will slowly reach the grass root level of prescribers. During this learning path, many prescribers will suffer from cognitive dissonance [8], i.e. evaluating biosimilars on the basis traditional drug development concept although being informed of biosimilarity. The mighty marketing machineries of pharmaceutical companies that are under threat of biosimilar competition seem to be very skilful in taking advantage of the non-rational aspects of prescription [9–12] in their campaign against biosimilars.
Time is money
The lifespan of a biosimilar that is a copy of a 10+ years old original product is limited. The market of biosimilars is eroded by influx of new products, including new ‘improved’ or ‘biobetter’ versions of the original product. While the benefits of the latter ‘convenience products’, such as the new, more concentrated formulation of original glargin insulin, are often marginal [13], aggressive marketing has managed to convince prescribers to switch patients to the new product that is protected against biosimilar competition. Thus, biosimilar glargin insulins have a negligible market share in most EU countries [14, 15]. In 2016, about half of the epoetin market and two thirds of the filgrastim market were protected by biobetters and subsequently biosimilars were able to take only a modest slice of the total epoetin alfa and filgrastim markets [1]. From the health economical point of view, biosimilars should be adopted to clinical use as soon as possible after marketing authorization in order to get the desired savings.
Interchangeability – suspicions without a smoking gun
Interchangeability is the key factor determining the success of biosimilars whose main market is in chronic treatment. Tendering processes have led to switches between biosimilars and the originator products in several countries without safety problems. Data from controlled and uncontrolled switches have not raised any safety, immunogenicity, or efficacy concerns [16, 17]. Many national regulatory agencies have issued position papers supporting physician-guided switches [18].
O’Brien et al. [19] described the process that led to the prescription of a biosimilar infliximab and later to the switching of the originator infliximab to the biosimilar infliximab in an Irish teaching hospital. This project lasted three years after licensing of the product and was based mainly on clinical studies and position papers. Even then, the hospital pioneered switching in Ireland where negative attitudes against switches are still common [20]. O’Brien et al. [19] predict that prescribers will also require switching studies from other biosimilars. This approach reflects the mistrust in the biosimilar development concept that aims to demonstrate physicochemical, structural, and functional similarity to the extent that the clinical performance will also be similar. Reliance on switch studies generates two problems. First, it will reduce the attractiveness of biosimilar development by increasing costs and narrowing the window of opportunity for biosimilars. Second, it is unlikely that reasonably sized switch studies will give reliable answers, as the potential differences in safety are small and significant problems very rare.
For the success of biosimilars, it will be critical whether clinicians will regard the clinical switching studies conducted thus far as the proof of concept or whether switching studies will always be required between an innovator product and its biosimilars or even between biosimilars of the same innovator product.
First, do not harm is a good principle for payers
Payers and policymakers have noticed the slow uptake of biosimilars and have taken measures to control pricing and prescription. Setting a minimum price reduction compared to the originator and requesting prescription quotas for biosimilars sound logical but may be counterproductive as they will reduce the attractiveness of the local market, especially in small Member States, to biosimilar developers. The market dynamics of biosimilars is different from that in generics market [21, 22]. In the Nordic countries, Denmark and Norway apply national tendering processes that have managed to introduce biosimilars relatively fast and obtained significant price reductions as compared to Finland that requires 30% price reduction and has to wait longer for biosimilars to enter the market. The situation is further complicated by different goals of companies developing biosimilars [1].
Companies developing only biosimilars are ready to price competition whereas for other companies also developing original biologicals, biosimilars are only the plan B. The latter companies do not readily enter price competition and wish to keep regulatory requirements high and competition low.
How about automatic substitution?
Successful use of generics required the introduction of automatic substitution. Several old beliefs of insurmountable problems in copying biological medicines, such as characterization of complex molecules, extrapolation of safety and efficacy, and interchangeability have turned out to be unfounded or greatly overstated. Now, it is time to have a second look at automatic substitution. Irrespective of their attitude to physician-guided interchangeability, position papers of medical societies and anti-biosimilar industry-sponsored publications state categorically that automatic substitution is not appropriate. Automatic substitution at the pharmacy level is currently not possible in most Member States [2, 23]. Larkin et al. [23] listed several prerequisites for automatic substitution, including additional clinical data and designation as an interchangeable biosimilar. Such a requirement will raise the bar for biosimilar development so high that only ‘Big Pharma’ can afford it and, thus, reduces competition. As always with biosimilars, discussion of automatic substitution is often biased by the interests of stakeholders.
What is the difference between physician-guided switching and automatic substitution?
There is a fairly wide consensus in the interchangeability of biosimilars [18]. Automatic substitution is a practical application of interchangeability that will be initiated at the political and administrative level when there are economic constraints and alternative ways to control costs are unpopular or harmful to public health. A prerequisite for automatic substitution is that the pharmacy staff will be able to provide information to patients and caregivers on biosimilars and, if necessary, training in the use of a new administration device. This is not an impossible hurdle for adequately staffed pharmacies. Another concern is traceability when a certain product is prescribed and later another is dispensed in the retail pharmacy. Information sharing between pharmacies, hospitals and prescribers outside hospitals may have to be improved to ensure traceability. This will require special arrangements that may include the development of local IT systems. These measures would be useful in improving traceability and adverse event reporting of biologicals in general. Thus, in most EU Member States, automatic substitution will require careful planning, sometimes changes to the legislation, and some support to pharmacies that will execute the substitution. A general scheme for the automatic substitution would be helpful and could be tailored for local circumstances in EU Member States.
Future of biosimilars
Prescribers and other healthcare professionals, patients, payers, and healthcare administrators are slowly learning the value and nature of biosimilars. Biosimilars will probably be adopted sooner in hospitals where the choice of the medicinal product is not an individual prescriber’s choice and where the budget determines the access to medicines.
The experience from the biosimilar glargin insulin suggests that the adoption of other biosimilars that are prescribed outside hospitals may be slow. Thus, additional measures, carrots and sticks, are needed. It seems likely that an increasing number of EU Member States will consider automatic substitution. Prescribers have to reconsider their role in ensuring the sustainability of the pharmacotherapy in EU – an active player or a bystander.
In the long run, biosimilars will become a standard tool for controlling costs of biologicals produced by biotechnology. The market dynamics of biosimilars is not straightforward and depends on the number of biosimilars coming to the market, as well as attitudes of payers and prescribers. Thus far, the method of restoring healthy competition seems to have been trial and error. In the future, EU Member States will probably adopt more harmonized approach to biosimilar pricing, reimbursement, procurement, prescribing and dispensing policies.
Competing interests: None.
Provenance and peer review: Commissioned; internally peer reviewed.
References
1. QuitilesIMS. The impact of biosimilar competition. May 2017 [homepage on the Internet]. [cited 2018 Mar 11]. Available from: http://www.medicinesforeurope.com/wp-content/uploads/2017/05/IMS-Biosimilar-2017_V9.pdf
2. Moorkens E, Vulto AG, Huys I, Dylst P, Godman B, Keuerleber S, et al. Policies for biosimilar uptake in Europe: an overview. PLoS One. 2017;12(12):e0190147.
3. Woodcock J. Keynote session. DIA/FDA Biosimilars Conference: Guidances, Science, and BsUFA. 12-13 September 2012, Washington DC, USA.
4. Annese V, Avendano-Sola C, Breedveld F, Ekman N, Giezen TJ, Gomollón F, et al. Roundtable on biosimilars with European regulators and medical societies, Brussels, Belgium. Generics and Biosimilars Initiative Journal (GaBI Journal). 2016;5(2):74-83. doi:10.5639/gabij.2016.0502.019
5. Danese S, Fiorino G, Raine T, Ferrante M, Kemp K, Kierkus J, et al. ECCO position statement on the use of biosimilars for inflammatory bowel disease – an update. J Crohns Colitis. 2017;11(1):26-34.
6. Tabernero J, Vyas M, Giuliani R, Arnold D, Cardoso F, Casali PG, et al. Biosimilars: a position paper of the European Society for Medical Oncology, with particular reference to oncology prescribers. ESMO Open. 2016;1(6):e000142.
7. Kay J, Schoels MM, Dörner T, Emery P, Kvien TK, Smolens JS, et al. Consensus-based recommendations for the use of biosimilars to treat rheumatological diseases. Ann Rheum Dis. 2018;77(2):165-74.
8. Phillips S. The evaluation of biosimilars and cognitive dissonance. BHBIA Yearbook. 2015;32.
9. Moorkens E, Jonker-Exler C, Huys I, Declerck P, Simoens S, Vulto AG. Overcoming barriers to the market access of biosimilars in the European Union: the case of biosimilar monoclonal antibodies. Front Pharmacol. 2016;7:193.
10. Avorn J. The psychology of clinical decision making – implications for medication use. N Engl J Med. 2018;378(8):689-91.
11. Albersheim SG, Golan A. The physician’s relationship with the pharmaceutical industry: caveat emptor…buyer beware! Isr Med Assoc J. 2011;13(7):389-93.
12. Lyles A. Biosimilars: patient and physician acceptability is the fifth hurdle to market competition. Generics and Biosimilars Initiative Journal (GaBI Journal). 2015;4(1):6-7. doi:10.5639/gabij.2015.0401.002
13. European Medicines Agency. Assessment report Abrasria. EMA/CHMP/340840/2014. 26 June 2014 [homepage on the Internet]. [cited 2018 Mar 11]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002835/WC500175383.pdf
14. GaBI Online – Generics and Biosimilars Initiative. Biosimilar insulins – reducing the cost of diabetes. [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2018 Mar 11]. Available from: www.gabionline.net/Biosimilars/Research/Biosimilar-insulins-reducing-the-cost-of-diabetes
15. Biogen. Attachment 1: How to maximize savings from biosimilars in Finland [homepage on the Internet]. [cited 2018 Mar 11]. Available from: https://www.eduskunta.fi/FI/vaski/JulkaisuMetatieto/Documents/EDK-2016-AK-86713.pdf
16. Cohen HP, Blauvelt A, Rifkin RM, Danese S, Gokhale SM, Woollet G. Switching reference medicines to biosimilars: a systematic literature review of clinical outcomes. Drugs. 2018. doi:10.1007/s40265-018-0881-y. Epub ahead of print
17. McKinnon RA, Cook M, Liauw W, Marabani M, Marschner IC, Packer NH, et al. Biosimilarity and interchangeability: principles and evidence: a systematic review. BioDrugs. 2018;32(1):27-52.
18. Medicines for Europe. Biosimilar medicines. Positioning statements on physician-led switching for biosimilar medicines Finland [homepage on the Internet]. [cited 2018 Mar 11]. Available from: http://www.medicinesforeurope.com/wp-content/uploads/2017/03/M-Biosimilars-Overview-of-positions-on-physician-led-switching.pdf
19. O’Brien G, Carroll D, Mulcahy M, Walshe V, Courtney G, Byrne S. Biosimilar infliximab introduction into the gastroenterology care pathway in a large acute Irish teaching hospital: a story behind the evidence. Generics and Biosimilars Initiative Journal (GaBI Journal). 2018;7(1):14-21. doi:10.5639/gabij.2018.0701.004
20. O’Callaghan J, Bermingham M, Leonard M, Hallinan F, Morris JM, Moore U, et al. Assessing awareness and attitudes of healthcare professionals on the use of biosimilar medicines: a survey of physicians and pharmacists in Ireland. Regul Toxicol Pharmacol. 2017;88:252-61.
21. Bocquet F, Loubière A, Fusier I, Cordonnier AL, Paubel P. Competition between biosimilars and patented biologics: learning from European and Japanese experience. Pharmacoeconomics. 2016;34:1173-86.
22. Rémuzat C, Dorey J, Cristeau O, Ionescu D, Radière G, Toumi M. Key drivers for market penetration of biosimilars in Europe. J Mark Access Health Policy. 2017;5(1):1272308.
23. Larkin H, Macdonald J, Lumsden R. Pharmacy-mediated substitution of biosimilars – a global survey benchmarking country substitution policies. Generics and Biosimilars Initiative Journal (GaBI Journal). 2017;6(4):157-64. doi:10.5639/gabij.2017.0604.034
Author Adjunct Professor Pekka Kurki, MD, PhD, University of Helsinki, 19 Lukupolku, FI-00680 Helsinki, Finland
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2018 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/eu-member-states-have-tools-to-reduce-costs-of-bestseller-biologicals-but-can-they-use-them.html