|
Aim: To explore whether medicines used in hospitals in European countries are supplied as originators or generic medicines, and to investigate the procurement conditions, including the extent of discounts at which the medicines are provided. |
Submitted: 3 July 2014; Revised: 29 November 2014; Accepted: 4 December 2014; Published online first: 17 December 2014
In recent years, policymakers in European countries have increased strategies to improve the uptake of generic medicines. For instance, INN prescribing (i.e. prescribing medicines by active ingredient rather than brand name), generics substitution (i.e. the practice of substituting a brand name medicine with a generic equivalent), and/or a reference price system (i.e. identical or similar medicines are clustered to a reference group, and the public payer defines the maximum amount – reference price – which is used as the basis for reimbursement for all medicines in the group), have been implemented in most countries of the European Union (EU) [1–8]. These policies to enhance the prescribing of generics versus on-patent medicines have, to a lesser or greater degree, been supplemented by further measures, typically in the outpatient sector, such as prescription monitoring and budgets, information campaigns to the public and, somewhat less frequently, financial incentives for pharmacists and patients [9–14].
This is done to ensure the provision of high-quality medicines at a lower financial burden for the payer, which is either the patient or the third party payer (social health insurance institutions or National Health Service). In many European countries, the latter covers, at least partially, the cost of medicines [7]. Generics are procured at, in some cases, considerably lower prices than originator medicines and thus contribute to savings for the payers, as seen in several countries, e.g. Sweden and Scotland [12, 15–20].
Pharmaceutical policy measures have usually focused on the outpatient sector. Pharmaceutical expenditure in hospitals has been fairly constant over the years (usually 5−10% of a nation’s medicines budget), so it has not been a priority of policymakers in European countries [21]. Knowledge of pharmaceutical policies, including procurement and funding strategies, in the hospital sector in Europe has therefore been limited. While clinical issues have been covered by a large body of literature, policy-related research has been scant [22]. However, in recent years, this has been changing because of an increasing awareness of the need to learn about hospital-related pharmaceutical policies [23] and to improve the management of pharmacotherapy at the interface of the inpatient and outpatient sectors. Several countries have launched initiatives in this field [24].
This information gap is partly related to dual organization and funding of the pharmaceutical systems in the European countries. Medicines prescribed and supplied in outpatient care are funded by the third-party payer, usually the state, while the remainder has to be co-paid by the patient. The third party payer decides, based on pharmacological, therapeutic and health economic considerations, which medicines used in outpatient care are reimbursed [7]. In the inpatient sector, except for special funding models for high-cost medicines, medicines are financed out of hospital budgets, which are funded by the hospital owners, which might be the state, regions, municipalities, religious orders, or some pooled funding from taxes and social health insurance contributions, depending on the country’s organization of healthcare services [25].
The outpatient and inpatient pharmaceutical systems tend to be seen as two distinct sectors within a country, hence the increasing focus on improving the interface management of pharmacotherapy. However, it is increasingly recognized that medication started during the hospital stay can impact the future medicines prescribed after a patient has been discharged [26–33]. It has been suggested that it might be better to supply, at favourable conditions, hospitals with off-patent medicines in order to ensure the initial prescribing with these medicines. However, as far as the authors know, no study has ever looked at the availability of originators and generic medicines at the level of individual hospitals in European countries. This is increasingly essential as more standard treatments lose their patents [34, 35].
Against this backdrop, this study sets out to explore whether medicines used in hospitals in European countries are supplied as on-patent or generic medicines. Furthermore, we aim to investigate the procurement conditions, including the extent of discounts at which the medicines are provided.
The analysis for this manuscript draws from data collected during the European Commission co-funded PHIS (Pharmaceutical Health Information System) project, which aimed to survey medicine management in hospitals in European countries and to collect prices of medicines used in hospitals (particularly on-patent medicines) [36, 37]. The methodology of this study was influenced by overall methodological decisions taken earlier in that project. For instance, the data collection was done for a larger basket of medicines, predominantly on-patent oncology medicines without generic alternatives.
Selection of medicines
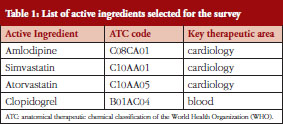
Out of a basket of medicines whose data we had surveyed, we selected those four molecules for which a ‘generic’ version was on the market. These were:
Table 1 provides the list of these four active ingredients indicating the ATC (Anatomical Therapeutic Chemical) code and the key therapeutic indication.
We included cardiovascular medicines because they account for high volumes in the outpatient sector, and the initial treatment in hospitals typically impacts further outpatient use [38].
At the time of the survey, the patent for clopidogrel had expired in some European countries, and not in others. In order to expand the study by another medicine not for cardiovascular treatment, we also included this blood product.
Selection of countries
We defined the following selection criteria for the countries, to ensure: 1) a geographic balance; 2) a balance between ‘old’ and ‘new’ EU Member States (acceded to the EU before and after May 2004) as well as European Economic Area (EEA)/European Free Trade Association (EFTA) countries; 3) a balance between countries with a social health insurance system and those with a general taxation-based system (national health service); 4) a balance between countries with a decentralized and a centralized procurement policy for medicines used in hospitals; and 5) a balance of countries of different economic situations. This is in line with cross-country comparisons available in the current literature [39].
Countries selected were Austria, The Netherlands, Norway, Portugal and Slovakia. We could not reach a balance in all cases, but we had countries from different geographic parts of Europe (criterion 1), at least one new EU Member State (Slovakia) and an EEA/EFTA country (Norway) (criterion 2), countries in different economic situations (criterion 5), and we had a balance regarding countries with a social health insurance system (Austria, The Netherlands, Slovakia) and those with a national health service (Portugal, Norway) (criterion 3). Centralized tendering for medicines in hospitals as a key procurement policy was organized in one country (Norway), and in two further countries it was done as a first step (Portugal) or for specific medicines (high-cost medicines; Slovakia) (criterion 4).
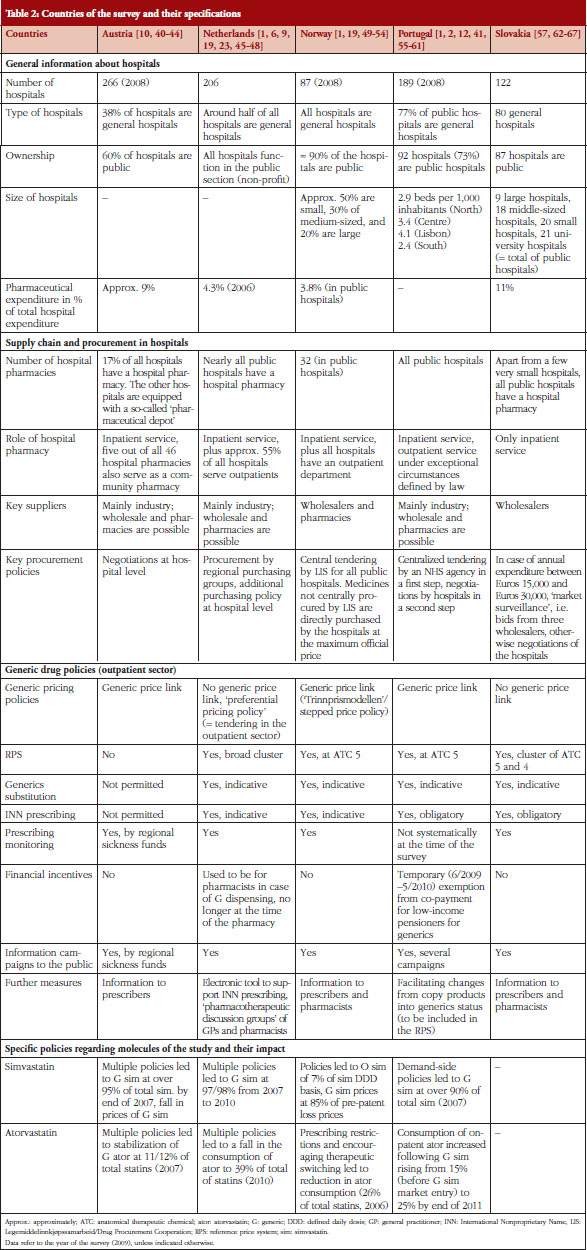
The selected countries had a variety of policies to enhance the prescribing and use of on-patent medicines versus generics. Table 2 provides an overview of country characteristics including their generic drug policies.
During the selection of the countries, country representatives (typically from pharmaceutical pricing and reimbursement authorities and national hospital pharmacy associations) involved in the PHIS (Pharmaceutical Health Information System) project as collaboration partners were addressed, and their support for the survey was sought. Thus, the willingness of the country representatives in our network was effectively an additional practical criterion for selection, and partially explains the selection of the countries, e.g. we did not manage to include a large country.
Survey instrument
A questionnaire was developed by the management team of the PHIS project, i.e. the authors and colleagues at their institutions. The draft methodology papers, including the questionnaire, were circulated with the PHIS Advisory Board (European Commission, Executive Agency for Health and Consumers, Eurostat, OECD, WHO Europe and WHO Headquarters) and the PHIS network members and then revised following their feedback. The methodology was piloted in two hospitals in Portugal and in one hospital in Austria, and adjustments to the questionnaire were based on the lessons learned from the pilot.
The questionnaire consisted of two parts: 1) a price survey form; and 2) a general questionnaire. The price survey form listed the selected molecules and asked for information about their availability, prices and procurement conditions in the hospitals. Information about the general availability in the country (marketing authorization) and price data for the outpatient sector (ex-factory prices for Austria, Portugal, Slovakia and pharmacy purchasing prices for The Netherlands and Norway) as of 30 September 2009 were already pre-filled with data provided by the Pharma Price Information (PPI) service of Gesundheit Österreich GmbH (Austrian Health Institute) [68]. Hospital pharmacists in the participating hospitals were asked to provide data as of 30 September 2009 on the availability, actual (real) prices at which medicines were supplied and procurement conditions, e.g. tendering processes versus direct negotiations, discounts, cost-free medicines, from the internal hospital databases. The general questionnaire contained questions about the medicines management in the surveyed hospitals.
Selection of the hospitals and data collection
The national network representatives were the ones identifying and approaching hospitals to explore their willingness to participate in the survey.
In Austria, The Netherlands, Norway and Portugal, we surveyed the data during study visits to the hospitals. Teams of at least two people, usually a researcher and a country’s representative involved in the PHIS network (from a competent authority for pharmaceutical pricing and reimbursement and/or a hospital pharmacy association), met with the hospital pharmacists and collected on site the information about the availability and procurement conditions (part 1 and 2 of the survey instrument). Only hospitals that had agreed in advance to participate in the survey were visited. Since none of the hospital pharmacists withdrew their cooperation during the study visit, the response rate was 100% in these countries.
In Slovakia, we had a mixed approach. We made study visits to three hospitals. In addition, we presented the project to hospital pharmacists during the general assembly of their national association and asked for their support by responding in writing to the price survey form and the questionnaire. Eight hospitals in Slovakia returned the filled price survey form and the questionnaire. This explains the considerably higher participation rate of hospitals in Slovakia compared with other countries.
We performed the study visits in the five countries and received the written questionnaires from Slovak hospitals between September 2009 and March 2010. On average, the study visits took about three hours per hospital1.
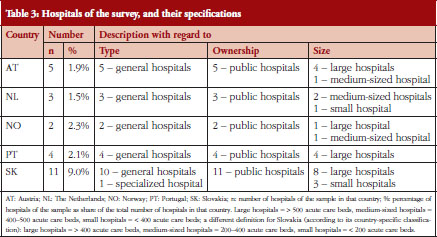
The survey results include data from five hospitals in Austria, three hospitals in The Netherlands, four hospitals in Portugal, two hospitals in Norway and eleven hospitals in Slovakia. We focused on general hospitals and on hospitals in public ownership. Most of the hospitals willing to participate were large hospitals, i.e. more than 500 acute care beds; or medium-sized hospitals, i.e. between 400 and 500 acute care beds. Table 3 provides an overview of the hospitals in the survey in relation to the total in the selected countries.
Data analysis
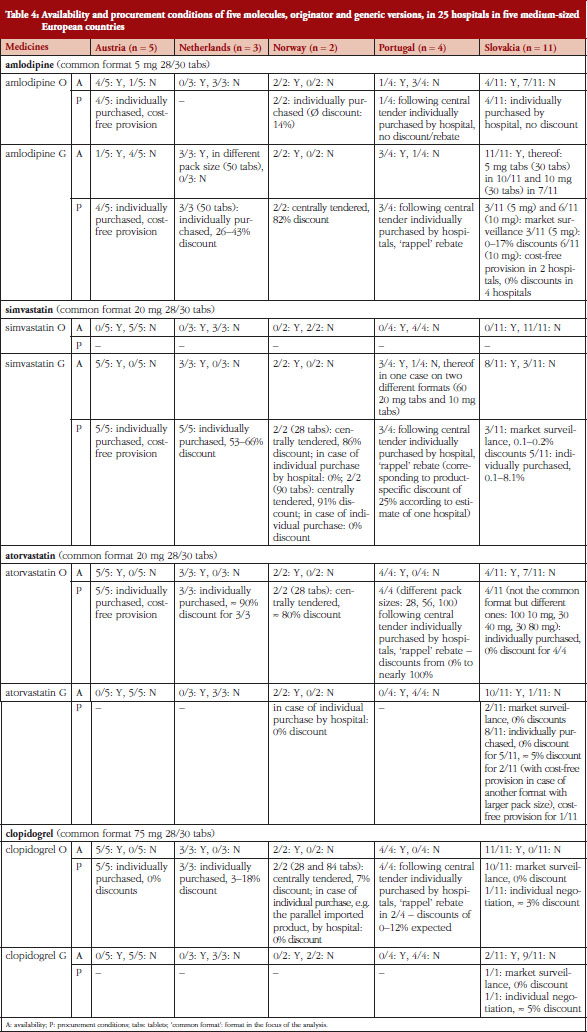
Data for all presentations (a presentation is defined as a medicine in a specific pharmaceutical form, dosage and pack size) of the four selected molecules supplied to the hospitals were collected. For the purpose of the analysis, we defined a ‘common presentation’, for which we performed the comparison of availability and procurement conditions. Findings about further presentations are also presented, see Table 4.
Terminology
This paper uses the terminology as defined in the glossary on pharmaceutical terms developed by the WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies [69]. Availability is defined as follows: The product is (physically) reachable for the patient, e.g. through the most accessible/appropriate healthcare supplier(s) at all times in adequate amounts and in the appropriate dosage forms, with assured quality and adequate information – so that patients have access to the medicine’. A discount is defined as ‘a price reduction granted to specified purchasers under specific conditions prior to purchase’, whereas a rebate is ‘a payment made to the purchaser after the transaction has occurred’. Country-specific terms for discounts and rebates, e.g. ‘rappel’ in Portugal, and procurement, e.g. ‘market surveillance’ in Slovakia, will be explained in the results section (see Table 4).
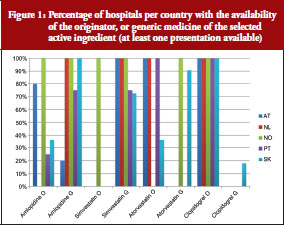
Figure 1 provides an overview of the availability of the selected medicines as originator or generic versions in the hospitals of the survey. Table 4 presents further information related to the procurement conditions, including the extent and types of discounts provided. Different procurement conditions surveyed were: cost-free provision, central tendering, market surveillance and individual purchase by the single hospital.
Variations were found between the countries and molecules: Hospitals in Norway, Slovakia and also Portugal and The Netherlands had the generics version more frequently available than did hospitals in Austria. Generic clopidogrel was only available in Slovakia, where the patent had already expired. Except for Norway, originator atorvastatin tended to be supplied to hospitals more frequently than the generic version, whereas simvastatin had the highest generic availability among the surveyed cardiovascular medicines across all countries. Except for Austria, amlodipine was preferably supplied as generic versions.
With the exception of one medicine in one hospital in Portugal, all surveyed hospitals had at least one presentation of the selected medicines. Hospitals in Austria, The Netherlands and Portugal always had exactly one presentation of the active ingredients, either originator or generic versions. In a few cases hospitals in Norway and Slovakia had both originator and the generic versions of the same presentation of a cardiovascular medicine. There was one hospital in Slovakia, which already had the generic version of clopidogrel, in addition to the originator.
Norway is the only country in which the surveyed medicines were exclusively centrally tendered, and the tendered presentations, independently whether they were originators or generics, were granted comparably high discounts. In Portugal, medicines used in hospitals were centrally tendered in a first step, during which an official tendering price to be valid for some years was set, and in a second step hospitals individually purchased the medicines they needed and could sometimes negotiate lower prices. In the other countries, hospitals individually procured the medicines from their suppliers, typically manufacturers and in very few cases wholesalers. For specific medicines, some hospitals in Slovakia used an instrument called ‘market surveillance’; i.e. a limited tendering process in which bids from three suppliers were requested and evaluated.
Discounts of 100% were observed in Austria (in the case of all three cardiovascular medicines in all hospitals) and in Slovakia (in very few cases) regardless of whether the originator or a generic version was supplied. A discount of 100% means that the medicines were provided to the hospital ‘cost-free’. Discounts in Portugal were difficult to assess at product level since they were granted in the form of a so-called ‘rappel’ during the purchase process of the hospital. Rappels are ex-post rebates, usually implemented at the end of the calendar year, with a bundling element, since they were granted to hospitals for a specific sales volume of all medicines of a supplier during a year.
The study looked at the availability of a small sample of medicines in hospitals in medium-sized European countries, to learn whether these medicines were available and in which form. We found that, with one exception, all surveyed medicines were available in all 25 surveyed hospitals. One hospital in Portugal did not have simvastatin; we were informed that the hospital had decided against procuring it since other medicines (atorvastatin) were considered sufficient as therapeutic choice.
The findings of our study, though exploratory due to the limited number of medicines and hospitals surveyed, highlight differences in availability between the outpatient and the hospital sectors. The selected medicines were marketed and were provided in community pharmacy in several different formats (different dosages and pack sizes) in the five countries (information provided by the PPI service [68]), but the hospitals usually had very few formats of a medicine, in most cases often exactly one format. This confirms that dispensing practices in hospitals are different than those in community pharmacies. In hospitals, single-dose packing is applied, whereas in the outpatient sector the full pack is dispensed to the patient who should then take the medication according to the instructions. In hospitals, therefore, medicines of a pack (large packs are purchased) are generally used for several patients.
Given the focused availability in hospitals, pharmaceutical companies are incentivized to be the sole supplier of a molecule to the hospitals. Even if the sales volume per product might be limited in the single hospitals, supplies for inpatients can be considered as strategically important for those medicines which will be used for long-term treatment in outpatient care after the patient’s discharge from hospital. Particularly if there are no or limited policies to enhance generics use in the outpatient sector (such as mandatory generics substitution, INN prescribing, information campaigns to the public, see Table 2 for an overview of these policies in the five countries), a change to the generic drug might be unlikely once treatment was started with an on-patent product. Reluctance by general practitioners to switch from the originator to a generic drug was even reported in Germany [70], a country with active generic drug promotion policy resulting in overall high generics uptake [71, 72]. Cardiovascular medicines, whose availability in hospitals we surveyed, are a typical example [27, 28, 38].
The stakeholders involved have conflicting objectives. Suppliers have a commercial interest to gain market shares, ideally to ensure sales volumes in the long run, whereas payers aim to keep costs down. Since several European countries have different public payers and/or different funding sources for the pharmaceutical bill in the outpatient and inpatient sectors [21, 22, 25, 63], the outpatient and inpatient payers are incentivized to shift treatments, patients, and costs from one sector to another. This is likely to impact the health outcomes of patients negatively, since such situations can irritate patients, and lead to medication errors [73–77].
Given these organizational and financial frameworks, the findings of our study are not surprising. Hospital pharmacists are under financial pressure to procure best prices within the existing pharmaceutical budgets, and they will thus purchase from those suppliers who offer the highest discounts. The purchasers’ approach is illustrated by the data that we collected on Austria. Austria is one of a few European countries in which cost-free provision of medicines to hospitals is allowed [22, 25, 40]. This procurement strategy is commonly used, at least for some medicines. In general, hospitals in Austria were not able to obtain discounts for new on-patent medicines, or to receive them as cost-free medicines [22, 25, 63, 78], but the five hospitals of the survey received the three cardiovascular medicines cost-free, two of which were originator brand-name medicines. We do not know whether generics manufacturers were in the position to offer as high discounts as the originator industry. Suppliers of originator medicines may benefit from longer-lasting business relationships with the hospitals and can adapt the marketing strategy in advance of patent expiry. Furthermore, suppliers that offer a range of medicines for different indications may be able to offer specific delivery conditions, including some kind of bundling. The cost-free provision of originator cardiovascular medicines in hospitals may considerably impact the continued use of originator medicines in outpatient care, particularly since Austria does not have INN prescribing, generics substitution or a reference price system [1]. Given the limited demand-side measures to enhance generics uptake, see Table 2, sickness funds (social health insurance institutions) as public payers for outpatient medication are required to constantly undertake information activities and prescribing monitoring. Due to dual financing, the key target groups are prescribers in the outpatient sector, and only recently sickness fund launched information activities addressing prescribers and staff in hospitals, however as a voluntary initiative, since social health insurance is not responsible for funding medicines in hospitals [10].
Stakeholders react in response to the incentives provided by the system. Interviews in Austria confirmed that hospital pharmacists were aware of the dilemma of supporting the start of a treatment with an originator medicine, but since they are responsible to their hospital administration, they will act in the best interest of the hospital.
The purchasing power of a single hospital might be questioned. Even if some hospitals might be able to obtain higher discounts, e.g. hospitals in Slovakia, overall the findings displayed rather small differences in discounts between the hospitals, and they suggested limited headroom of the individual hospitals to negotiate large price reductions. Central tendering is likely to be connected with stronger purchasing power. Norway has decided that medicines for all public hospitals are centrally procured by the public procurement agency LIS (Legemiddelinnkjøpssamarbeid, Drug Procurement Cooperation). LIS defines preferred presentations and tenders for them. Medicines not tendered by LIS, e.g. different pack sizes, dosages, can be purchased individually by the hospitals [49]. The data from our survey showed that LIS tended to define a generic as a preferred version of the surveyed cardiovascular medicines. It was reported that hospitals in Norway had individually purchased some other ‘non-preferred’ presentations of these molecules, and they were not granted any discounts. The example of Norway could be considered as good practice since it combines financial elements with awareness-raising activities targeting prescribers. LIS staff have performed extensive information activities in hospitals to inform doctors about the defined presentations, and the rationale behind for selecting them. At the same time, the practice highlights the relevance of financial incentives that, in the case of Norway, support measures to enhance generics use in hospitals. In a country such as Austria, on the other hand, generics promotion activities of hospital pharmacists (via the Drugs and Therapeutics Committee, for instance, and their generics substitution which has been performed in hospitals for years but is not permitted in the outpatient sector) [40] are less effective since a limited number of generics are available due to cost-free provision of the originators to hospitals.
We also included clopidogrel in the basket of surveyed medicines even if the patent had only expired in Slovakia at the time of the survey. We learned in the interviews that hospital pharmacists in the other countries were eagerly awaiting the patent expiry because they aimed to change to the generics version as soon as possible, and obtain larger discounts and even cost-free provision in the case of Austria. However, hospital pharmacists might not see their expectations fulfilled given the controversy regarding generic clopidogrel, which was launched as a different salt with fewer indications initially [79, 80].
Our study has several limitations. A major limitation concerns the small basket of medicines, with only three cardiovascular medicines plus clopidogrel, which is still patented in most of the countries studied. In addition, the number of hospitals varied among the countries and was low in some countries. We were not always able to obtain complete information on the procurement conditions, particularly on the discounts, since in Portugal the ‘rappel’, an ex-post bundling rebate, allowed at best estimates on the product-specific price reductions. Some limitations were related to the medicine procurement system in a country, such as the Portuguese ‘rappel’. Also, this study was a follow-up of a larger study within the PHIS project, in which we surveyed more medicines, particularly on-patent medicines without any generic alternatives. The overall setting of the EU funded PHIS project has, to a large extent, contributed to some methodological decisions. Competent authorities and hospital pharmacists, who were already members of the PHIS network, were involved as cooperation partners in the survey, and not academics. Finally, we acknowledge that the study focused on the aspect of procurement of medicines to hospitals and, though we discussed the implications of the supply of originators and generics versions for the overall healthcare system, in the light of existing generic drug policies in the outpatient sector, the issue of improving use of generics was not within the scope of this study.
Therefore, this study can only be considered as an exploratory piece of research. We recommend repeating the survey, applying the same survey design, but with a larger basket of medicines (including medicines with generics available due to recently expired patents) and including more hospitals and countries.
Notwithstanding its limitations, the study provides important new evidence. Medicines procurement policies and management in European hospitals have been overlooked by researchers and policymakers for a long time, and the investigation of pharmaceutical policies in the inpatient sector has been called for [23]. To our knowledge, the availability of originator and generic medicines in European hospitals has never been surveyed. In the EU and other high-income countries, including the US and Australia, studies on the availability of medicines have been limited to the outpatient sector, and availability not measured at the level of the single healthcare provider (pharmacy, retailer) but at the national level [81, 82]. Primary data collected on availability and prices of medicines in single healthcare units and dispensaries (e.g. hospitals, clinics, pharmacies, and retailers) have been performed based on the WHO/HAI methodology [83] in some low- and middle-income countries [84, 85] but not in high-income countries. We were able to survey additional data about the procurement conditions; particularly discounts and rebates considered as confidential information.
The study confirms the general availability of the selected medicines, and, at the same time, highlights the strategy of hospitals to be focused on one or a few presentations of a molecule. If generic alternatives are available, generics tend to be supplied to the hospitals but this is not always the case. Cardiovascular medicines, which were studied in this survey, are of relevance for both industry and public payers, since they account for high volumes due to high patient numbers and long-term use. The initial treatment in hospitals is likely to impact further medicine use in the outpatient sector and to result in a continuation of the same brand, especially if pharmaceutical policies do not encourage a switch to a generic version. The study provides a good starting point to learn about originator and generic medicines use in hospitals. The findings suggest the need to develop policies that support a more integrative healthcare system, e.g. via joint funding models for the outpatient and inpatient sectors, in order to improve medicine management at the interface of outpatient and inpatient sectors.
For patients it is important to obtain the medical treatment they require. Availability of and access to medicines is one major element. The selected medicines were found to be available in the surveyed hospitals.
Generics provide an opportunity for a more rational use of medicines and for savings to public payers. Starting treatment with generics in the hospitals would be appreciated: public payers would achieve savings, and patients would continue in outpatient care with the medication they started. The study showed that in case of the generics alternatives available these are used in some but not all hospitals. In addition, the study suggests the need for improved pharmaceutical policies at the interface of the outpatient and inpatient sectors. Limited interface management directly impacts patients in a negative way, and can contribute to confusion, irritation and even deteriorated health outcomes of the patient.
We thank the hospital pharmacists of the 25 hospitals for their willingness to participate in this study. We are very grateful that they took the time to answer our questions during the interviews and that they shared with us the data which were of confidential character in most cases. Since we assured anonymity to the hospitals concerned, we do not disclose the names of data providers. We are grateful to our (former) colleagues Claudia Habl, Christine Leopold and Simone Gritsch (Gesundheit Österreich GmbH), and Barbara Bilancikova (SUKL) for their involvement in the methodology development and survey at the time of the PHIS (Pharmaceutical Health Information System) project. We thank the PHIS Advisory Board (Jérôme Boehm, Artur Furtado, Aders Lamark Tysse, Giulia del Brenna, Christophe Roeland, Stefaan van der Spiegel of the European Commission; Anna Thuvander, Jurgita Kaminskaite of the (then) Executive Agency for Health and Consumers, Dorota Kawiorska of Eurostat, Elizabeth Docteur, Valérie Paris of OECD, Kees de Joncheere of WHO Regional Office for Europe, Richard Laing and Dele Abegunde of WHO Headquarters – institutional affiliations refer to the time of the PHIS project) as well as the PHIS network members for their feedback to draft methodology papers. In particular, we greatly appreciate the support of the PHIS network members of selected countries in identifying and addressing hospitals for cooperation.
Competing interests: The authors have no reported conflicts of interest. The methodology development and the survey was done within the framework of the PHIS (Pharmaceutical Health Information System) project that was commissioned by the Executive Agency for Health and Consumers (EAHC) under the call for proposals 2007 in the priority area ‘health information’ of the European Commission, Directorate-General Public Health and Consumers, and was co-funded by the Austrian Federal Ministry of Health.
As a follow-up of the PHIS project, we analysed the data of medicines with a generic version available with regard to their availability and procurement conditions, and we prepared this manuscript. No separate funding was provided for the supplementary analysis regarding the research question and the drafting of this manuscript.
Provenance and peer review: Commissioned; externally peer reviewed.
Sabine Vogler1, PhD
Nina Zimmermann1, MA
Jan Mazag2, PharmaDr
1WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies, Health Economics Department, Gesundheit Österreich GmbH/Österreichisches Bundesinstitut für Gesundheitswesen (GÖG/ÖBIG, Austrian Health Institute), 6 Stubenring, AT-1010 Vienna, Austria
2Statny Ustav pre Kontrolu Lieciv (SUKL, State Institute for Drug Control), 11 Kvetná, SL-82508, Bratislava 26, Slovakia
References
1. Vogler S. The impact of pharmaceutical pricing and reimbursement policies on generics uptake: implementation of policy options on generics in 29 European countries–an overview. Generics and Biosimilars Initiative (GaBI Journal). 2012;1(2):93-100. doi: 10.5639/gabij.2012.0102.020
2. Vogler S, Zimmermann N, Leopold C, de Joncheere K. Pharmaceutical policies in European countries in response to the global financial crisis. South Med Review. 2011;4(2):69-79.
3. Leopold C, Vogler S, Habl C. Was macht ein erfolgreiches Referenzpreissystem aus? Erfahrungen aus internationaler Sicht [in German]/Implementing a successful reference price system – experiences from other countries. Soziale Sicherheit. 2008(11):614-23.
4. Dylst P, Vulto A, Godman B, Simoens S. Generic medicines: solutions for a sustainable drug market? Appl Health Econ Health Policy. 2013;11(5): 437-43.
5. Simoens S. A review of generic medicine pricing in Europe. Generics and Biosimilars Initiative Journal (GaBI Journal). 2012;1(1):8-12. doi:10.5639/gabij.2012.0101.004
6. Dylst P, Simoens S, Vulto A. Reference pricing systems in Europe: characteristics and consequences. Generics and Biosimilars Initiative Journal (GaBI Journal). 2012;1:127-31. doi:10.5639/gabij.2012.0103-4.028
7. Vogler S, Habl C, Bogut M, Voncina L. Comparing pharmaceutical pricing and reimbursement policies in Croatia to the European Union Member States. Croat Med J. 2011;52(2):183-97.
8. Simoens S. Trends in generic prescribing and dispensing in Europe. Expert Rev Clin Pharmacol. 2008 Jul;1(4):497-503.
9. Dylst P, Vulto A, Simoens S. Demand-side policies to encourage the use of generic medicines: an overview. Expert Rev Pharmacoecon Outcomes Res. 2013;13(1):59-72.
10. Vogler S, Zimmermann N. How do regional sickness funds encourage more rational use of medicines, including the increase of generic uptake? A case study from Austria. Generics and Biosimilars Initiative Journal (GaBI Journal). 2013;2(2):65-75. doi:10.5639/gabij.2013.0202.027
11. Godman B, Shrank W, Wattermark B, Andersen M, Bishop I, Gustafsson LL. Use of generics – a critical cost containment measure for all healthcare professionals in Europe? Pharmaceuticals. 2010;3(8):2470-94.
12. Godman B, Shrank W, Andersen M, Berg C, Bishop I, Burkhardt T, et al. Comparing policies to enhance prescribing effi ciency in Europe through increasing generic utilization: changes seen and global implications. Expert Rev Pharmacoecon Outcomes Res. 2010;10(6):707-22.
13. Godman B, Shrank W, Andersen M, Berg C, Bishop I, Burkhardt T, et al. Policies to enhance prescribing effi ciency in Europe: fi ndings and future implications. Front Pharmacol. 2010;1:141.
14. Godman B, Wettermark B, Bishop I, Burkhardt T, Fürst J, Garuoliene K, et al. European payer initiatives to reduce prescribing costs through use of generics. Generics and Biosimilars Initiative Journal (GaBI Journal). 2012;1(1):22-7. doi:10.5639/gabij.2012.0101.007
15. World Health Organization. Cameron A, Laing R. Cost savings of switching private sector consumption from originator brand medicines to generic equivalents. World Health Report. Background Paper, 35. Geneva 2010 [homepage on the Internet]. 2011 Sep 17 [cited 2014 Nov 15]. Available from: http://www.who.int/healthsystems/topics/financing/healthreport/35MedicineCostSavings.pdf
16. Seeley E, Kanavos P. Generic medicines from a societal perspective: savings for health care systems? Eurohealth. 2008;14(2):18-21.
17. Simoens S. International comparison of generic medicine prices. Curr Med Res Opin. 2007;23(11):2647-54.
18. Tafuri G, Creese A, Reggi V. National and international differences in the prices of branded and unbranded medicines. Journal of Generic Medicines. 2004;1(2):120-7.
19. Vogler S. How large are the differences between originator and generic prices? Analysis of five molecules in 16 European countries. Farmeconomia Health economics and therapeutic pathways. 2012;13 (Suppl 3):29-41.
20. Bennie M, Godman B, Bishop I, Campbell S. Multiple initiatives continue to enhance the prescribing efficiency for the proton pump inhibitors and statins in Scotland. Expert Rev Pharmacoecon Outcomes Res. 2012;12(1):125-30.
21. Vogler S, Zimmermann N, Mazag J. Procuring medicines in hospitals: results of the European PHIS survey. Eur J Hosp Pharm Prac. 2011(2):20-1.
22. Vogler S, Zimmermann N, Habl C, Mazag J. The role of discounts and loss leaders in medicine procurement in Austrian hospitals – a primary survey of official and actual medicine prices. Cost Eff Resour Alloc. 2013;11(1):15.
23. Vogler S, Habl C, Leopold C, Rosian-Schikuta I. PPRI Report. Vienna: Gesundheit Österreich GmbH/Geschäftsbereich ÖBIG, 2008. 2008 Jun 2 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/BooksReports/PPRI_Report_final.pdf
24. Björkhem-Bergman L, Andersén-Karlsson E, Laing R, Diogene E, Melien O, Jirlow M, et al. Interface management of pharmacotherapy. Joint hospital and primary care drug recommendations. Eur J Clin Pharmacol. 2013;69(1):73-8.
25. Vogler S, Habl C, Leopold C, Mazag J, Morak S, Zimmermann N. PHIS Hospital Pharma Report. Vienna: Pharmaceutical Health Information System (PHIS); commissioned by the European Commission and the Austran Federal Ministry of Health, 2010. 2010 Jul 16 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/BooksReports/PHIS_HospitalPharma_Report.pdf
26. Perren A, Donghi D, Marone C, Cerutti B. Economic burden of unjustified medications at hospital discharge. Swiss Med Wkly. 2009;139(29-30):430-5.
27. Gallini A, Legal R, Taboulet F. The influence of drug use in university hospitals on the pharmaceutical consumption in their surrounding communities. Br J Clin Pharmacol. 2013;75(4):1142-8.
28. Feely J, Chan R, McManus J, O’Shea B. The infl uence of hospital-based prescribers on prescribing in general practice. Pharmacoeconomics. 1999;16(2):175-81.
29. Schröder-Bernhardi D, Dietlein G. Lipid-lowering therapy: do hospitals influence the prescribing behavior of general practitioners? Int J Clin Pharmacol Ther. 2002;40(7):317-21.
30. Himmel W, Tabache M, Kochen M. What happens to long-term medication when general practice patients are referred to hospital? Eur J Clin Pharmacol. 1996;50(4):253-7.
31. Himmel W, Kochen M, Sorns U, Hummers-Pradier E. Drug changes at the interface between primary and secondary care. Int J Clin Pharmacol Ther. 2004;42(2):103-9.
32. Grimmsmann T, Schwabe U, Himmel W. The infl uence of hospitalisation on drug prescription in primary care–a large-scale follow-up study. Eur J Clin Pharmacol. 2007;63(8):783-90.
33. Bijl D, Van Sonderen E, Haaijer-Ruskamp F. Prescription changes and drug costs at the interface between primary and specialist care. Eur J Clin Pharmacol. 1998;54(4):333-6.
34. Frank RG. The ongoing regulation of generic drugs. N Engl J Med. 2007;357(20):1993-6.
35. Jack A. Balancing Big Pharma’s books. BMJ. 2008;336(7641):418-9.
36. Hoebert J, Mantel-Teuwisse A. PHIS Evaluation Report. Utrecht: Pharmaceutical Health Information System (PHIS), 2011. 2011 Apr 6 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/FurtherDocuments/PHIS evaluation report.pdf
37. Vogler S, Leopold C, Zimmermann N, Habl C, de Joncheere K. The Pharmaceutical Pricing and Reimbursement Information (PPRI) initiative–experiences from engaging with pharmaceutical policy makers. Health Policy and Technology. 2014;3(2):139-48.
38. de Vries CS, van Diepen NM, Tromp TF, de Jong-van den Berg LT. Auditing GPs’ prescribing habits: cardiovascular prescribing frequently continues medication initiated by specialists. Eur J Clin Pharmacol. 1996;50(5):349-52.
39. Cacace M, Ettelt S, Mays N, Nolte E. Assessing quality in cross-country comparisons of health systems and policies: towards a set of generic quality criteria. Health Policy. 2013;112(1-2):156-62.
40. Zimmermann N, Vogler S. PHIS Hospital Pharma Report Austria. Vienna: Pharmaceutical Health Information System (PHIS), 2009. 2009 Jun 30 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationReports/PHIS_Hospital_Pharma_AT_Report_Final_version_090630.pdf
41. Vogler S, Zimmermann N. The potential of generics policies: more room for exploitation–PPRI Conference Report. Generics and Biosimilars Initiative Journal (GaBI Journal). 2012;1(3-4):146-9. doi:10.5639/gabij.2012.0103-4.030
42. Leopold C, Habl C, Vogler S, Morak S. PPRI Pharma Profi le Austria. Vienna: Pharmaceutical Pricing and Reimbursement Information (PPRI), 2008. 2008 Nov 13 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformation/Reports/Austria_PPRI_2008_Englih_Version.pdf
43. Winkelmayer WC, Asslaber M, Bucsics A, Burkhardt T, Schautzer A, Wieninger P, et al. Impact of reimbursement changes on statin use among patients with diabetes in Austria. Wien Klin Wochenschr. 2010;122(3-4):89-94.
44. Godman B, Burkhardt T, Bucsics A, Wettermark B, Wieninger P. Impact of recent reforms in Austria on utilization and expenditure of PPIs and lipidlowering drugs: implications for the future. Expert Rev Pharmacoecon Outcomes Res. 2009;9(5):475-84.
45. Storms H, Schreurs M. PHIS Hospital Pharma Report The Netherlands Vienna: Pharmaceutical Health Information System (PHIS), 2010. 2010 May 10 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationReports/PHISNLHospital Pharma Report 2009.pdf
46. Dylst P, Vulto A, Simoens S. Tendering for outpatient prescription pharmaceuticals: what can be learned from current practices in Europe? Health Policy. 2011;101(2):146-52.
47. Dylst P, Simoens S. Generic medicine pricing policies in Europe: current status and impact. Pharmaceuticals. 2010;3(3):471-81.
48. Woerkom Mv, Piepenbrink H, Godman B, Metz Jd, Campbell S, Bennie M, et al. Ongoing measures to enhance the effi ciency of prescribing of proton pump inhibitors and statins in The Netherlands: infl uence and future implications. J Comp Eff Res. 2012;1(6):527-38.
49. Aanes T, Ognøy AH, Festøy H. PHIS Hospital Pharma Report Norway. Vienna: Pharmaceutical Health Information System (PHIS), 2009. 2009 Nov 3 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationReports/PHISNorway Hospital Pharma Report 2009.pdf
50. Festöy H, Sveen K, Leung-Ming Y, Gjönnes L, Gregersen T. PPRI Pharma Profile Norway. Vienna: Pharmaceutical Pricing and Reimbursement Information (PPRI), 2008. 2009 Mar 9 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationReports/ Norway_
PPRI_2008.pdf
51. Håkonsen H, Horn AM, Toverud E-L. Price control as a strategy for pharmaceutical cost containment – what has been achieved in Norway in the period 1994-2004? Health Policy. 2009;90(2-3):277-85.
52. Brekke KR, Holm TH, Straume OR. Margins and market shares: pharmacy incentives for generic substitution. European Econ Rev. 2013;61:116-31.
53. Godman B, Sakshaug S, Berg C, Wettermark B, Haycox A. Combination of prescribing restrictions and policies to engineer low prices to reduce reimbursement costs. Expert Rev Pharmacoecon Outcomes Res. 2011;11(1):121-9.
54. Sakshaug S, Furu K, Karlstad Ø, Rønning M, Skurtveit S. Switching statins in Norway after new reimbursement policy: a nationwide prescription study. Br J Clin Pharmacol. 2007;64(4):476-81.
55. Caldeira S, Furtado C, Vieira I, Baptista A. PHIS Hospital Pharma Report Portugal Vienna: Pharmaceutical Health Information System (PHIS), 2010. 2011 Mar 10 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationReports/PHIS Hospital Pharma Portugal 2010.pdf
56. Teixeira I, Vieira I. PPRI Pharma Profile. Portugal. Vienna: PPRI (Pharmaceutical Pricing and Reimbursement Information), 2008. 2008 Dec 16 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationReports/Portugal_PPRI_2008.pdf
57. Leopold C, Mantel-Teeuwisse AK, Vogler S, Valkova S, de Joncheere K, Leufkens HG, et al. Effect of the economic recession on pharmaceutical policy and medicine sales in eight European countries. Bull World Health Organ. 2014;92(9):630-40.
58. Simoens S. The Portuguese generic medicines market: a policy analysis. Pharm Pract (Granada). 2009;7(2):74-80.
59. Leopold C, Zhang F, Mantel-Teeuwisse AK, Vogler S, Valkova S, Ross-Degnan D, et al. Impact of pharmaceutical policy interventions on utilization of antipsychotic medicines in Finland and Portugal in times of economic recession: interrupted time series analyses. Int J Equity Health. 2014;13:53.
60. Habl C, Vogler S, Leopold C, Schmickl B, Fröschl B. Referenzpreissysteme in Europa. Analyse und Umsetzungsvoraussetzungen für Österreich. Wien: ÖBIG Forschungs- und Planungsgesellschaft mbH; 2008. 2008 Apr 11 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/BooksReports/EB_RPS_31_3_08.pdf
61. Quintal C, Mendes P. Underuse of generic medicines in Portugal: an empirical study on the perceptions and attitudes of patients and pharmacists. Health policy. 2012;104(1):61-8.
62. Mazag J. PHIS Hospital Pharma Report Slovakia. Vienna: Pharmaceutical Health Information System (PHIS), 2009. 2009 Aug 13 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformation Reports/7SlovakiaHospital Pharma.pdf
63. Vogler S, Zimmermann N, Leopold C, Habl C, Mazag J. Discounts and rebates granted for medicines for hospital use in fi ve European countries. The Open Pharmacoeconomics and Health Economics Journal. 2013;5:1-10.
64. Mazag J, Segec A. PPRI Pharma Profi le Slovakia. Vienna: Pharmaceutical Pricing and Reimbursement Information (PPRI), 2007. 2007 May 11 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/CountryInformationReports/Slovakia_PPRI_2007.pdf
65. Kaló Z, Docteur E, Moïse P. Pharmaceutical pricing and reimbursement policies in Slovakia. Paris: OECD, 2008. [cited 2014 Nov 15]. Available from: http://dx.doi.org/10.1787/244264621247
66. Håkonsen H, Toverud E-L. A review of patient perspectives on generics substitution: what are the challenges for optimal drug use. Generics and Biosimilars Initiative Journal (GaBI Journal). 2012;1(1):28-32. doi:10.5639/gabij.2012.0101.008
67. Palagyi M, Lassanova M. Patients attitudes towards experience with use of generics in Slovakia, performance of generic substitution. Bratisl Lek Listy. 2008;109(7):324-8.
68. Gesundheit Österreich GmbH. Pharma Price Information (PPI) service. Vienna 2014. [cited 2014 Nov 15]. Available from: http://www.goeg.at/en/PPI
69. WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies. Glossary of pharmaceutical terms. Update 2013. Vienna 2013 [homepage on the Internet]. 2013 Nov 25 [cited 2014 Nov 15]. Available from: http://whocc.goeg.at/Literaturliste/Dokumente/MethodologyTemplate/PHISGlossary_Update2013_fi nal_gesamt.pdf
70. Simmenroth-Nayda A, Hummers-Pradier E, Ledig T, Jansen R, Niebling W, Bjerre LM, et al. Prescription of generic drugs in general practice. Results of a survey of general practitioners [Article in German]. Med Klin (Munich). 2006;101(9):705-10.
71. Godman B, Schwabe U, Selke G, Wettermark B. Update of recent reforms in Germany to enhance the quality and efficiency of prescribing of proton pump inhibitors and lipid-lowering drugs. Pharmacoeconomics. 2009;27(5):435-8.
72. Garattini L, Tediosi F. A comparative analysis of generics markets in five European countries. Health Policy. 2000;51(3):149-62.
73. Gleason K, McDaniel MR, Feinglass J, Baker D, Lindquist L, Liss D, et al. Results of the Medications At Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25(5):441-7.
74. Glintborg B, Andersen SE, Dalhoff K. Insuffi cient communication about medication use at the interface between hospital and primary care. Qual Saf Health Care. 2007;16(1):34-9.
75. Layson-Wolf C, Morgan JA. Pharmacy continuity of care: what do community pharmacists need from an acute care hospital to improve continuity of pharmaceutical care? Disease Management and Health Outcomes. 2008;16(4): 199-203.
76. Santell JP. Reconciliation failures lead to medication errors. Jt Comm J Qual Patient Saf. 2006;32(4):225-9.
77. Vira T, Colquhoun M, Etchells E. Reconcilable differences: correcting medication errors at hospital admission and discharge. Qual Saf Health Care. 2006;15(2):122-6.
78. Langebner T. Managing drug costs in Austria. Eur J Hosp Pharm Prac. 2007;13(5):79.
79. Baumgartel C, Godman B, Malmstrom R, et al. What lessons can be learned from the launch of generic clopidogrel? Generics and Biosimilars Initiative Journal (GaBI Journal). 2012;1(2):58-68. doi:10.5639/gabij.2012.0102.016
80. Baumgärtel C. Generic clopidogrel–the medicines agency’s perspective. Generics and Biosimilars Initiative Journal (GaBI Journal). 2012;1(2):89-91. doi:10.5639/gabij.2012.0102.019
81. Danzon PM, Furukawa MF. Prices and availability of pharmaceuticals: evidence from nine countries. 2003;Suppl Web Exclusives:W3-521-36.
82. Danzon PM, Furukawa MF. International prices and availability of pharmaceuticals in 2005. Health Aff (Milwood). 2008;27(1):221-33.
83. World Health Organization. Measuring medicine prices, availability, affordability and price components. Geneva: WHO, 2008 [homepage on the Internet]. 2013 May 6 [cited 2014 Nov 15]. Available from: http://www.haiweb.org/medicineprices/manual/manuals/MedicinePrices.pdf
84. Cameron A, Ewen M, Ross-Degnan D, Ball D, Laing R. Medicine prices, availability, and affordability in 36 developing and middle-income countries: a secondary analysis. Lancet. 2009;373(9659):240-9.
85. Mendis S, Fukino K, Cameron A, Laing R, Filipe Jr A, Khatib O, et al. The availability and affordability of selected essential medicines for chronic diseases in six low-and middle-income countries. Bull World Health Organ. 2007;85(4):279-88.
| Author for correspondence: Sabine Vogler, PhD, Head of WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies, Health Economics Department, Gesundheit Österreich GmbH/Österreichisches Bundesinstitut für Gesundheitswesen (GÖG/ÖBIG, Austrian Health Institute), 6 Stubenring, AT-1010 Vienna, Austria |
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2014 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Source URL: https://gabi-journal.net/availability-and-procurement-conditions-of-originator-and-generic-medicines-in-hospitals-an-exploratory-study-in-five-medium-sized-european-countries.html
Copyright ©2025 GaBI Journal unless otherwise noted.