Comparative efficacy studies of biosimilars: data versus theoretical risks, beliefs, and comfort
Published on 2024/04/19
Generics and Biosimilars Initiative Journal (GaBI Journal). 2024;13(1):23-6.
|
Abstract: |
Submitted: 8 April 2024; Revised: 18 April 2024; Accepted: 19 April 2024; Published online first: 29 April 2024
Introduction
Biological therapies are rapidly advancing scientifically. Gene and cell therapies have already entered the clinic. However, the success story of biologicals is overshadowed by the high costs that are increasingly limiting access to life-saving medicines [1].
The costs of chemically synthesized medicines dramatically drop following the introduction of generic equivalents, after the exclusivity period. Biosimilars are copies of biologicals that can also, in principle, reduce the costs of off-patent biologicals. Unfortunately, biosimilars have not succeeded in fulfilling their potential. There are several reasons for their poor performance.
The unwillingness of prescribers to prescribe and switch to biosimilars has delayed the growth of the biosimilar market. Resistance remains despite availability of scientific and educational publications on the safety and efficacy of biosimilars. It seems obvious that the hesitance is due to non-scientific reasons such as misinformation, administrative burden, worries about physician autonomy, and lack of incentives [2]. Therefore, several countries have adopted or are planning to adopt automatic substitution policies and tendering to promote rational use of biologicals.
The other main reason for the high prices of biosimilars is lack of competition caused by two main factors. Namely, these are the anti-competitive measures put in place by the innovator industry, such as questionable patents, and the stringent regulatory requirements for biosimilars leading to high development costs [3–5]. The regulatory guidelines for biosimilars in the European Union, US and elsewhere were initially very conservative. They have been revised over time but remain stringent. The main factors contributing to the high development costs include purchasing the reference comparator biological products and running controlled efficacy trials with large patient samples to demonstrate clinical equivalence. The stringent regulatory requirements are expected to constrain the ability of current manufacturers to develop biosimilars needed for rare diseases, and new manufacturers to develop products and join the competition [4]. This paper aims to clarify as what is already known about the role of large clinical efficacy studies and the ongoing re-evaluation of their future role in biosimilar development.
The role of large efficacy and safety studies in biosimilar development
The current guidelines of European Medicines Agency (EMA) and US Food and Drug Administration (FDA) allow some flexibility in designing the clinical development of biosimilars but in practice, a comparative efficacy trial with clinical efficacy endpoint can only be avoided by conducting a pharmacodynamic (PK) study with a marker that is an established surrogate of efficacy. Such pharmacodynamic (PD) markers are not available for most biosimilars, notably monoclonal antibodies (mAbs). This means that, without revision of the guidelines, even more efficacy studies will be conducted in future as most new biosimilars will be mAbs or their derivatives. Thus, controlled efficacy studies are not only expensive but will also strain the clinical research resources of hospitals which may delay the development of new innovative medicines, especially in oncology.
Long-term safety of biosimilars
At the inception of biosimilar guidelines and products, there were many uncertainties. The long-term safety and efficacy of biosimilars has been surprisingly good, considering their current widespread use. None of the theoretical worries, including issues related to immunogenicity and extrapolation of therapeutic indications, have yielded post-licensing issues [6–9]. Thus, the development concept of biosimilars has been validated. The remaining question is whether all parts of the development; analytical, in vitro functional tests, in vivo non-clinical models, human PK and PD studies, as well as comparative efficacy and safety studies, provide useful information. Analytical and in vitro functional testing, as well as clinical PK/PD studies do provide unique information, whereas the in vivo non-clinical toxicology studies are considered useless [7]. Comparative efficacy (and safety) studies have been called ‘confirmatory’ but are increasingly controversial.
Are large efficacy/safety studies necessary?
The conduct of clinical efficacy and safety studies is regarded as the gold standard in the development of new innovative medicines. The requirement of comparative clinical efficacy studies in the development of biosimilars is deeply rooted in the minds of many clinicians and regulators. Several retrospective studies have been conducted to estimate the impact of efficacy studies on the approvability of biosimilars [10–15]. The studies covered all products approved 2006–2019 [10, 11] or focused on the more complex molecules, mAb and fusion proteins [12–14]. Data were extracted from public assessment reports, mainly from the European Public Assessment Reports. It was revealed that controlled efficacy studies did not significantly contribute to the regulatory decision-making process and that they are insensitive to significant analytic and in vitro functional differences. In general, products that were comparable in analytical, in vitro functional, and PK studies were approved irrespectively of the outcome of the comparable efficacy study.
There were two cases of increased immunogenicity due to leachables from the syringe epoetin-α and host cell impurities (somatropin). These problems can be avoided in the future as our experience of developing and evaluation of biosimilars has increased. The performance of analytical methods and our understanding of structure function relationships have improved over time. Differences in the active substances did not trigger significant differences in immunogenicity between the biosimilar and the reference product.
There were two cases where the candidate biosimilar was rejected due to a lack of analytical comparability, even though the clinical efficacy study met the equivalence criteria. There were three products that were comparable in analytical and in vitro functional tests and/or PK study but the comparative efficacy study failed to demonstrate equivalence. In these cases, post hoc analyses of the efficacy data led to the approval. In conclusion, comparative efficacy studies do not significantly affect regulatory decision-making. Thus, it is doubtful whether clinical efficacy studies can be called ‘confirmatory’ for biosimilarity because of their lower sensitivity for significant differences. Post-marketing surveillance is the only feasible way to detect rare serious adverse effects.
Confirmatory efficacy studies: are regulatory dominos falling?
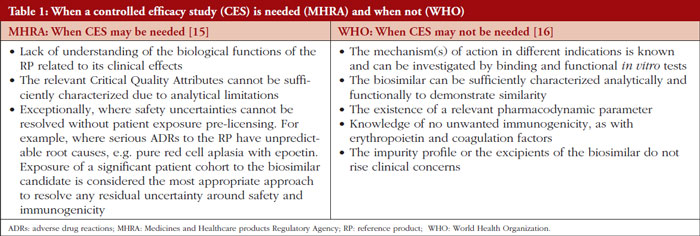
UK regulatory agency Medicines and Healthcare products Regulatory Agency (MHRA) and the World Health Organization (WHO) have revised their biosimilar guidelines by listing factors that may justify the conduct of a powered efficacy study [15, 16]. Using these criteria, manufacturers may ask for a waiver of the comparative efficacy study, see Table 1. It is expected that, using these criteria, comparative efficacy studies will be exceptional in the development of conventional biosimilar therapeutic proteins. Thus, the goal is not the categorical elimination of controlled efficacy studies, especially in development of new types of complex biosimilars or proteins that have serious unpredictable adverse effects.
EMA’s Biosimilar Medicines Working Party (BMWP) of the Committee of Human Medicinal Products (CHMP) has issued a concept paper that proposes drafting a reflection paper for re-evaluation of the need for comparative efficacy studies [17]. Several former and current BMWP experts have published scientific articles supporting the reduction of comparative efficacy studies and some participated in drafting the WHO guideline. [13, 14, 16, 18] Thus, it would be surprising if the reflection paper would not recommend the revision of the CHMP guidelines according to the current knowledge of the role of powered efficacy studies in the development of biosimilars.
FDA appears to be the most conservative major regulatory agency. FDA has a rather flexible guidance concerning comparative efficacy trials in biosimilar development, but it has been applied in a conservative manner. The interchangeability designation is an additional hurdle, as it may be difficult to reduce comparative efficacy studies if companies must conduct large comparative switching studies to obtain the designation. The main clinical concern of FDA seems to be immunogenicity. FDA experts published a thorough review of interchangeability studies [19]. The conclusion was that no difference was found in the safety profiles or immunogenicity rates in patients who were switched and those who remained on a reference biological. This study, together with several previous reviews, questions the scientific and ethical justification of switch studies.
FDA hosted a workshop of The Biosimilar Working Group of International Pharmaceutical Regulators Programme (IPRP) in September 2023, to discuss the need for comparative efficacy studies in biosimilar development [20]. Regulators representing ‘stringent’ agencies had a broad agreement in the need for re-evaluation of the role of comparative efficacy studies, but no concrete international consensus efforts were proposed. WHO and MHRA presented their models for reducing comparative efficacy studies. EMA announced the ongoing process for revision of its guidance on comparative efficacy studies. FDA had more reservations which were explained by the ‘newness’ of the biosimilar concept and the difficulty of reversing the strong historical attachment to comparative efficacy studies — the gold standard for innovative medicines. In addition, FDA seems not to be entirely convinced in the extrapolation of historical evidence to future biosimilars. Instead, FDA has a research programme aiming to find innovative ways to simplify biosimilar development, such as biomarkers, PD markers, new statistical methods, testing drug formulations, and better understanding of the clinical significance of differences in the analytical and in vitro functional tests, as well as possibilities to predict immunogenicity by in silico and in vitro methodologies [21]. These efforts may benefit the development of biological medicines in general. However, the finding and validation of the potential new methods for demonstration of biosimilarity may take years.
Pharmaceutical regulation should serve public health
Some medicines regulatory agencies are streamlining their requirements while others are hesitating. Experts from the biosimilar industry argue that the necessary data for revision and harmonization of regulatory guidance are already available [22]. This situation raises increasing concerns among payers and policymakers in the US and elsewhere about increasing costs of biological therapy. In fact, the US budget proposal for 2025 includes a legislative initiative to ‘Eliminate the Statutory Distinction between the Approval Standard for Biosimilar and Interchangeable Biosimilar Products and Deem that Approved Biosimilars are Interchangeable’ [23]. This would be in line with the statement of EMA and the Heads of Medicines Agencies in the EU and might pave the way for reduction of comparative efficacy studies.
According to the pharmaceutical legislation in the EU, the essential aim of the regulation of medicinal products must be to safeguard public health [24]. However, this goal must be attained by means which will not hinder the development of the pharmaceutical industry or trade in medicinal products within the Community. These principles fit well in the discussion about comparative efficacy studies. Increased competition will lead to better access to important medicines and removal of redundant efficacy studies will allow new companies to initiate biosimilar development.
It is obvious that the reduction of comparative efficacy studies would trigger criticism among parts of the industry that are afraid of increasing competition. Prescribers are used to relying on comparative efficacy studies and have still difficulties in understanding the concept of biosimilarity. Thus, they may be shocked if the ‘confirming’ (in fact comforting) comparative efficacy studies are not required anymore for all biosimilars. Therefore, regulators need to ally with learned societies that have issued position papers on biosimilars and have the authority to explain the data on the true role of ‘confirmatory’ efficacy studies. Even then, automatic substitution may become necessary to speed up the acceptance of the revised biosimilar development concept.
Many important therapeutic proteins have recently lost the exclusivity or will lose it soon [25]. Thus, regulators should not miss the opportunity to simplify and accelerate the development of new biosimilars. EMA and FDA should strive to a common or at least compatible position with WHO and MHRA on the role of comparative efficacy studies and the interchangeability concept. This would increase harmonization of key regulatory requirements without an arduous ICH-type harmonization process.
Disclaimer
The author alone is responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which he is affiliated.
Funding sources
No funding was received to write this article.
Competing interests: The author declares no conflicts of interest.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
1. Makurvet FD. Biologics vs. small molecules: drug costs and patient access. Med Drug Discov. 2021;9:100075.
2. Sarnola K, Merikoski M, Jyrkkä J, Hämeen-Anttila K. Physicians’ perceptions of the uptake of biosimilars: a systematic review. BMJ Open. 2020;10(5):e034183.
3. Chen BK, Yang YT, Bennett CL. Why biologics and biosimilars remain so expensive: despite two wins for biosimilars, the Supreme Court’s recent rulings do not solve fundamental barriers to competition. Drugs. 2018;78(17):1777-81.
4. IQVIA. Assessing the biosimilar void achieving sustainable levels of biosimilar competition in Europe. 2023 [homepage on the Internet]. [cited 2024 Apr 18]. Available from:https://www.iqvia.com/insights/the-iqvia-institute/reports-and-publications/reports/assessing-the-biosimilar-void
5. Fontanillo M, Körs B, Alex Monnard A. Three imperatives for R&D in biosimilars. McKinsey & Company. 19 August 2022. Available from: https://www.mckinsey.com/industries/life-sciences/our-insights/three-imperatives-for-r-and-d-in-biosimilars
6. Kurki P, Barry S, Bourges I, Tsantili P, Wolff-Holz E. Safety, immunogenicity and interchangeability of biosimilar monoclonal antibodies and fusion proteins: a regulatory perspective. Drugs. 2021;81(16):1881-96.
7. Kurki P, Kang HN, Ekman N, Knezevic I, Weise M, Wolff-Holz E. Regulatory evaluation of biosimilars: refinement of principles based on the scientific evidence and clinical experience. BioDrugs. 2022;36(3):359-71.
8. Nikitina V, Santi Laurini G, Montanaro N, Motola D. Comparative safety profiles of oncology biosimilars vs. originators in Europe: an analysis of the EudraVigilance Database. Cancers (Basel). 2023;15(14):3680.
9. Sagi S, Anjaneya P, Kalsekar S, Kottke A, Cohen HP. Long-term real-world post-approval safety data of multiple biosimilars from one marketing-authorization holder after more than 18 years since their first biosimilar launch. Drug Saf. 2023;46(12):1391-404.
10. Webster CJ, Wong AC, Woollett GR. An efficient development paradigm for biosimilars. BioDrugs. 2019;33:603-11.
11. Schiestl M, Ranganna G, Watson K, Jung B, Roth K, Capsius B, et al. The path towards a tailored clinical biosimilar development. BioDrugs. 2020;34(3):297-306.
12. Bielsky MC, Cook A, Wallington A, Exley A, Kauser S, Hay JL et al. Streamlined approval of biosimilars: moving on from the confirmatory efficacy trial. Drug Discov Today. 2020:S1359-6446(20)30343-3.
13. Guillen E, Ekman N, Barry S, Weise M, Wolff-Holz E. A data driven approach to support tailored clinical programs for biosimilar monoclonal antibodies. Clin Pharmacol Ther. 2023;113(1):108-23.
14. Kirsch-Stefan N, Guillen E, Ekman NV, Barry S, Knippel V, Killalea S, et al. Do the outcomes of clinical efficacy trials matter in regulatory decision-making for biosimilars? BioDrugs. 2023;37:855-71.
15. Medicines & Healthcare products Regulatory Agency. Guidance on the licensing of biosimilar products. 2022 [homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://www.gov.uk/government/publications/guidance-on-the-licensing-of-biosimilar-products/guidance-on-the-licensing-of-biosimilar-products
16. World Health Organization. Guidelines on evaluation of biosimilars. Replacement of annex 2 of WHO technical report series, no.977. 2022 [homepage on the Internet]. [cited 2024 Apr 18]. Available from:https://www.who.int/publications/m/item/guidelines-on-evaluation-of-biosimilars
17. European Medicines Agency. Concept paper for the development of a Reflection Paper on a tailored clinical approach in biosimilar development [homepage on the Internet]. [cited 2024 Apr 18]. Available from:https://www.ema.europa.eu/en/documents/other/concept-paper-development-reflection-paper-tailored-clinical-approach-biosimilar-development_en.pdf
18. Wolff-Holz E, Tiitso K, Vleminckx C, Weise M. Evolution of the EU biosimilar framework: past and future. BioDrugs. 2019;33(6):621-34.
19. Herndon TM, Ausin C, Brahme NN, Schrieber SJ, Luo M, Andrada FC, et al. Safety outcomes when switching between biosimilars and reference biologics: a systematic review and meta-analysis. PLoS One. 2023;18(10):e0292231.
20. U.S. Food and Drug Administration. IPRP Biosimilars Working Group Workshop: ‘Increasing the efficiency of biosimilar development programs re-evaluating the need for comparative Clinical Efficacy Studies (CES)’13 September 2023 [homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://www.fda.gov/media/172198/download
21. U.S. Food and Drug Administration. BsUFA III Regulatory Research Pilot Program: Research Roadmap [ homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://www.fda.gov/media/164751/download
22. Cohen HP, Turner M, McCabe D, Woollett GR. Future evolution of biosimilar development by application of current science and available evidence: the developer’s perspective. BioDrugs. 2023;37(5):583-93.
23. U.S. Food and Drug Administration. FY25 Legislative proposals [homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://www.fda.gov/media/176924/download?attachment
24. EUR-Lex. Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001 on the Community code relating to medicinal products for human use [homepage on the Internet]. [cited 2024 Apr 18]. Available from: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32001L0083
25. Troien P, Newton M, Scott K, Mulligan C. The impact of biosimilar competition in Europe. IQVIA Report 2021. Available from: https://www.iqvia.com/-/media/iqvia/pdfs/library/white-papers/the-impact-of-biosimilar-competition-in-europe-2021.pdf
|
Author: Adjunct Professor Pekka Kurki, MD, PhD, University of Helsinki, 19 Lukupolku, FI-00680 Helsinki, Finland |
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2024 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.


