Canadian prescribers’ attitudes and perceptions about ophthalmic biosimilars
Published on 2023/05/04
Generics and Biosimilars Initiative Journal (GaBI Journal). 2023;12(2):41-9.
Author byline as per print journal: Michael S Reilly, Esq; Jane Barratt, PhD
|
Introduction: The first biosimilar entered the Canadian market in 2009 and the first ophthalmic biosimilar was approved in 2022. In 2022, the Alliance for Safe Biologic Medicines (ASBM) and the International Federation on Ageing (IFA) asked prescribing ophthalmology physicians in Canada for their views on product identification, prescribing biologicals and prescribing biosimilars and switching. |
Submitted: 24 February 2023; Revised: 25 April 2023; Accepted: 26 April 2023; Published online first: 9 May 2023
Introduction
In Canada, the first biosimilar product approved by Health Canada entered the market in 2009, this was Sandoz’s growth hormone treatment Omnitrope (somatropin) [1, 2]. By June 2022, 50 biosimilar products had been approved in Canada [2, 3]. This includes the first ophthalmology biosimilar, Byooviz (SB11), approved in 2022 and produced by Samsung Bioepis and commercialized by Biogen which is a biosimilar of Genentech (Roche)/Novartis’ blockbuster eye drug Lucentis (ranibizumab) [4].
India paved the way for ophthalmology biosimilars, with the first ophthalmic biosimilar of ranibizumab approved in 2015 (Razumab, Intas Pharmaceuticals Ltd, Ahmedabad, Gujarat, India) [5, 6]. Following expiry of the originator patents in regions across the world, Byooviz has been the first ophthalmology biosimilar to be approved in regions such as Europe, the US and Canada [7, 8].
The introduction of anti-vascular endothelium-derived growth factors (anti-VEGF), such as ranibizumab, for the treatment of various retinal vascular diseases has transformed ophthalmology. Now that biosimilars of these drug products are available or are in the pipeline, they have the potential to impact more patients worldwide by offering more affordable treatment options [6].
Ranibizumab inhibits angiogenesis (the formation of new blood vessels) by inhibiting VEGF-A. Ranibizumab can be used to treat macular degeneration by inhibiting VEGF, which is responsible for the excessive formation of blood vessels in the retina leading to progressive loss of vision. The monoclonal antibody drug is indicated for the treatment of wet age-related macular degeneration (AMD), macular oedema, degenerative myopia and diabetes complications; all conditions of the eye causing vision loss [9].
The use of compounded bevacizumab in ophthalmology is widespread globally [6, 10]. However, the application of this biological is off-label as, for example in the US, the product is FDA-approved to treat colorectal cancer, and it has not been through the rigorous FDA process required for approval to treat ophthalmic pathology [11]. Compounded ziv-aflibercept is also used off-label despite intravitreal use being contraindicated in the EU because of its hyperosmotic properties [12]. The compounding of these products for use in retinal diseases may also increase the risk of intraocular infections [13–16]. Although biosimilars of these products have been approved or are in the pipeline, the US American Academy of Ophthalmology (AAO) advises against the use of biosimilars of these products in ophthalmology as they have not been studied for ophthalmic indications and their inactive ingredients have not all been approved for use in the eye [17, 18].
A survey carried out by the International Retina Biosimilar Study Group (Inter BIOS Group) revealed that many retinal physicians from Europe and the US have concerns regarding the safety and efficacy of biosimilars [19]. Due to the off-label use of biologicals in this field, the concern may be well founded. However, biosimilar products of biologicals that are approved for ocular treatment should not pose a problem as regulators have very robust tests to determine biosimilarity that allow any clinically meaningful differences between originators and potential biosimilars to be determined, and this is also true for anti-VEGF biosimilars, such as ranibizumab [10]. In January 2022, the AAO issued a policy statement on the biosimilars in ophthalmologic use [17]. The guideline outlines that, for an ophthalmic biosimilar, a comparative clinical trial is generally required in addition to a similarity comparison, and this includes extensive pharmacokinetic and pharmacodynamic analysis with phase III equivalence studies where appropriate [11]. The acceptance and use of biosimilars is key in the field of ophthalmology as they can reduce the cost of care for debilitating eye diseases and increase access to treatment globally.
Many provinces of Canada have adopted a switching policy wherein patients are switched from expensive originator products to lower-cost approved biosimilar versions of the drug. Such policy decisions are made in a bid to drive down healthcare costs and increase access to treatment however they have been met with some opposition [20]. Such switching policies may influence the opinion of ophthalmology practitioners in Canada regarding biosimilars.
In 2022, the Alliance for Safe Biologic Medicines (ASBM) commissioned a web-based survey to be conducted by ophthalmology practitioners/physicians across Canada. This was designed to document ophthalmologist perspectives on: identification of biologicals/biosimilars (by brand name, non-proprietary name or DIN) and the reporting of adverse drug events related to them; the cost of biologicals and biosimilars and how this may influence if they are prescribed; prescribing biosimilars and switching to biosimilars; pharmacist-level switching to biosimilars and automatic substitution of biosimilars.
This survey was very similar to those previously carried out in Australia [21], Europe [22, 23], South America [24] and the US [25–27) that asked for prescriber opinions on prescribing practices, naming and labelling of biologicals, switching and substitution and the interchangeability designation.
Sample characteristics and methodology
In October/November 2022 the ASBM conducted a web-based survey of 41 ophthalmology practitioners in Canada.
Low sample size was a function of finding not just ophthalmologists, but those who are retinal specialists in Canada (those who prescribe biologicals). These are a new specialty in which biosimilars are becoming available; results are consistent with other ASBM physicians’ surveys conducted in Australia, Canada, Europe, Latin America and the US using identical methodology and questions.
Survey respondents are from Industry Standard Research’s (ISR) contracted partner’s commercially available physician panel that covers more than 70 countries worldwide. They receive between US$25 and US$75 for survey participation, depending on specialty and geography.
The physician panel provider uses their internal database of more than 1,000,000 healthcare professionals worldwide for sampling. Also, when necessary, the physician panel provider partners with other market research companies to meet the demands of healthcare clients in the industry. The market research companies go through very selective vetting processes as well as training on ISO certification and market research industry standards to make sure all provide the best service to clients.
ISR’s physician panel provider uses the following channels for recruitment:
- Professional conferences
- Direct Mail
- Online recruitment
- Email, fax, mailing lists of verified market research companies.
All survey respondents are managed online through the market research companies’ patented, internal, proprietary system, which is ISO 26362 certified since 2011.
The questionnaires were developed as a collaboration between ASBM and IFA management and membership, and ISR management. No ‘validation’ has been conducted as the instruments do not measure higher level ‘constructs’. They are purely direct measures of opinion and attitude.
Details of respondent profile
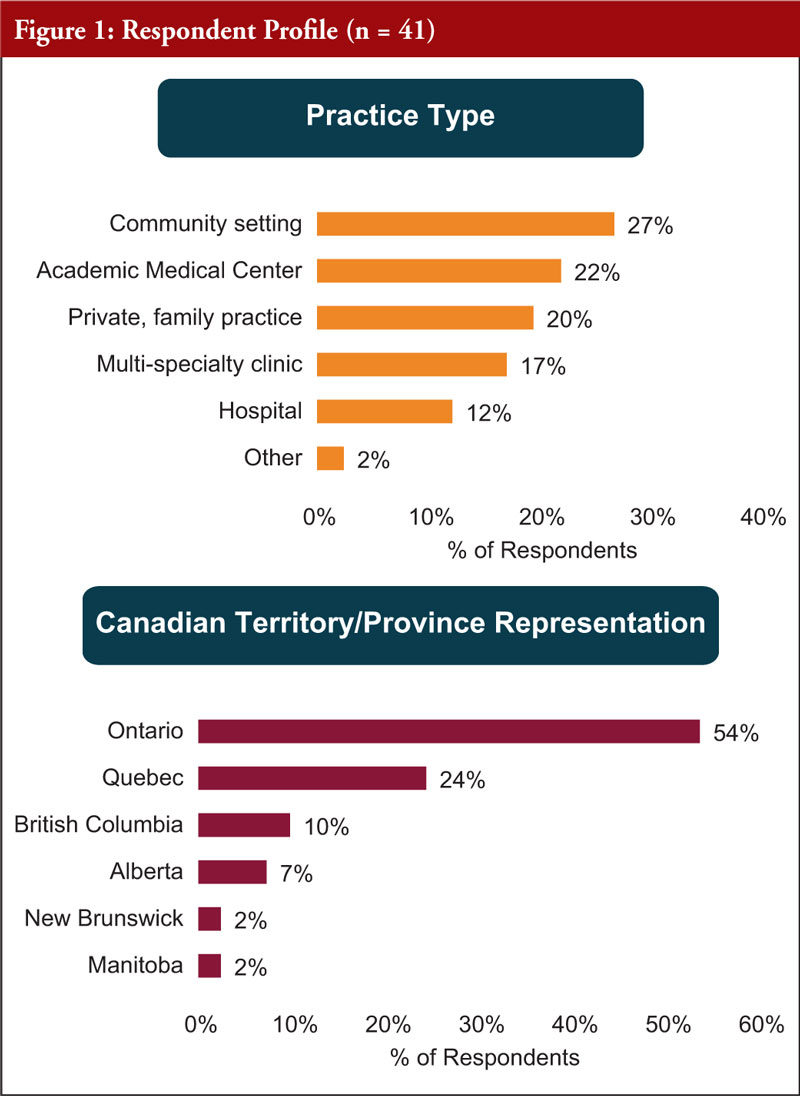
The participants worked in a number of different practice types, including: the community setting, academic medical practice, private family practice, multi-specialty clinics and hospitals. They came from the provinces of: Ontario, Quebec, British Colombia (BC), Alberta, New Brunswick and Manitoba. With the majority (54%) coming from Ontario, and just under a quarter (24%) from Quebec, see Figure 1.
All participants (100%) said they prescribe biologicals. Regarding the knowledge of biosimilars, the vast majority of participants (95%) said they were either very familiar, with a complete understanding of them, or familiar with a basic understanding, however 2% did say they had never heard of biosimilars, see Figure 2.
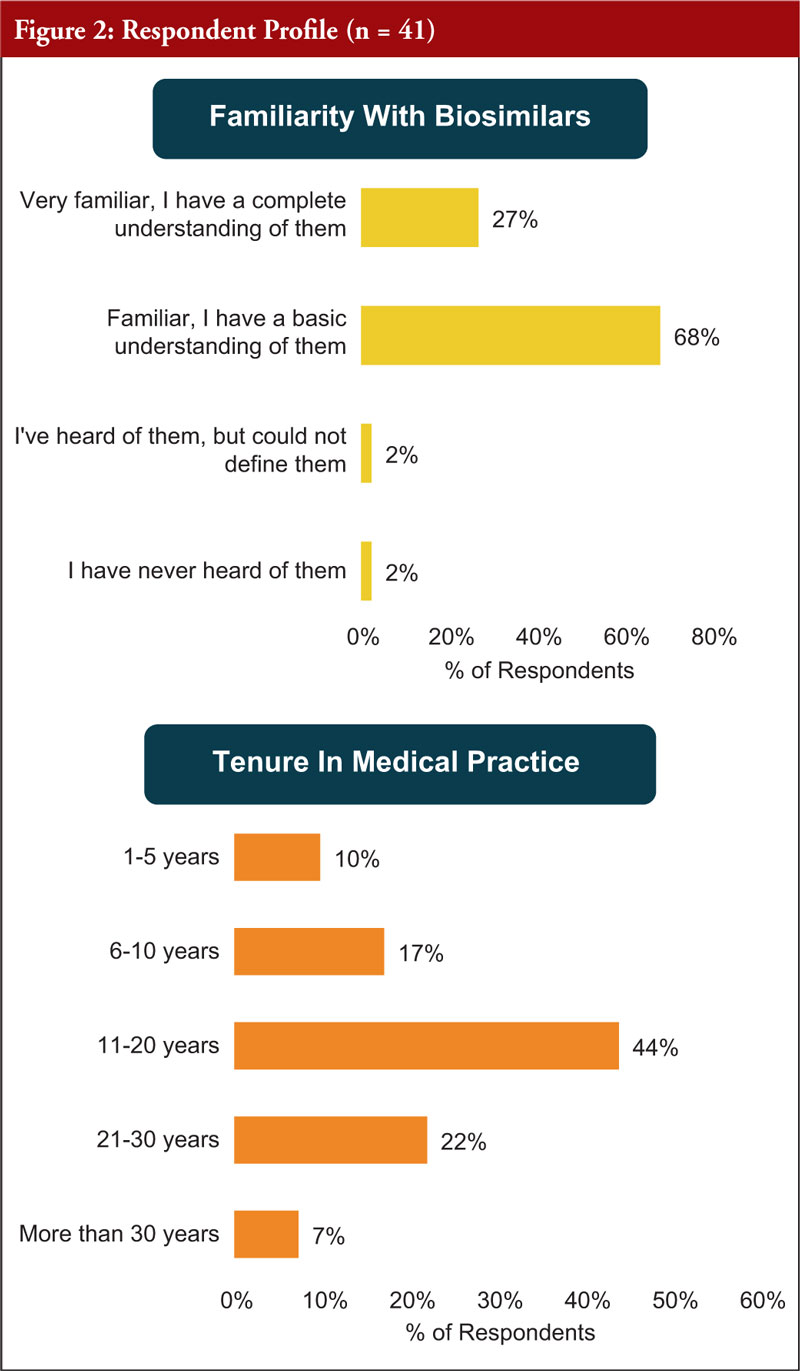
With regards to tenure in medical practice, most participants (44%) have been practicing for between 11–20 years, whilst 27% have been practicing for under 11 years and 29% have been practicing for over 20 years.
Online survey
Prescribers were asked to consider:
- When identifying a prescription of a biological drug in patient records, are they likely to identify the medicine by their product/brand name or their non-proprietary/generic name.
- In the context of identifying a biological for purposes of reporting an adverse event, are they likely to identify the medicine by their product/brand name, non-proprietary/generic name or DIN number.
- Confidence levels in the Canadian pharmacovigilance system’s ability to accurately identify the specific product, at the brand-name level, that might be responsible for an adverse drug reaction.
- How often they include the lot/batch number when recording adverse drug reactions.
- The reasons for not including the lot/batch number when recording adverse drug reactions (relevant to prescribers who rarely or never include the lot/batch number only).
- If they would support Health Canada harmonizing internationally by adopting a distinct suffix system.
- How costs to the public system impact which biological drug they prescribe.
- If cost to the public system were not a factor, how would that impact their choice of originator biological vs biosimilar prescription (relevant only to those who were impacted by the cost of biologicals to the public system).
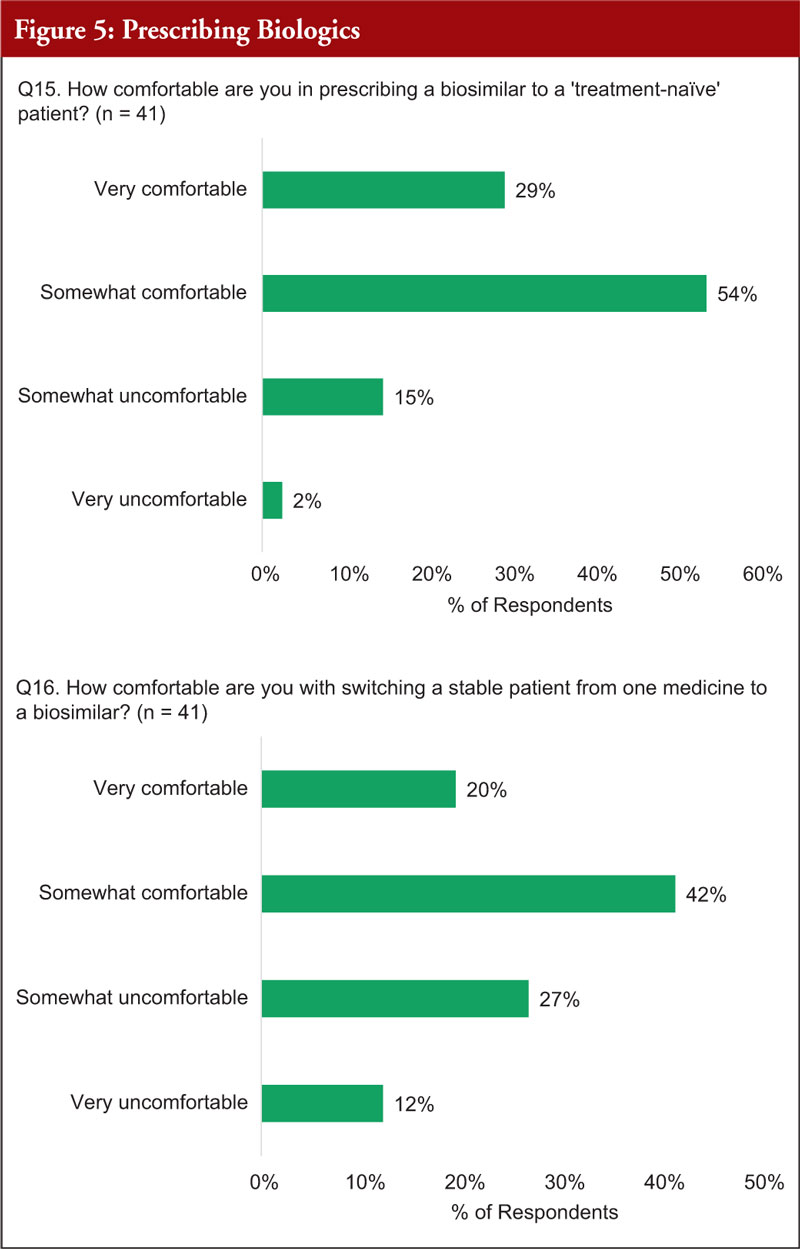
- Their comfort levels: a) prescribing a biosimilar to a ‘treatment-naïve’ patient; and b) switching a stable patient from one medicine to a biosimilar.
- How they are influenced by the quality of a biological’s patient support program.
- The importance of patient education on biosimilars prior to switching a patient to a biosimilar.
- The importance of having the authority to designate a biological medicine as ‘DISPENSE AS WRITTEN’ or ‘DO NOT SUBSTITUTE’, when: a) faced with a situation where substitution by a pharmacist; or b) faced with a situation where it is permissible for payer (public or private) to require a patient who is stable on their current biological to switch to a biosimilar.
- The importance of a) being notified by the pharmacist that a patient has received a biological other than the one prescribed, if the patient was receiving chronic (repeated) treatment; and b) having the sole authority to decide, together with patients, the most suitable biological medicine for their disease.
- How acceptable it would be if the pharmacist made the determination which biological (originator or biosimilar) to dispense to a patient on initiation of treatment.
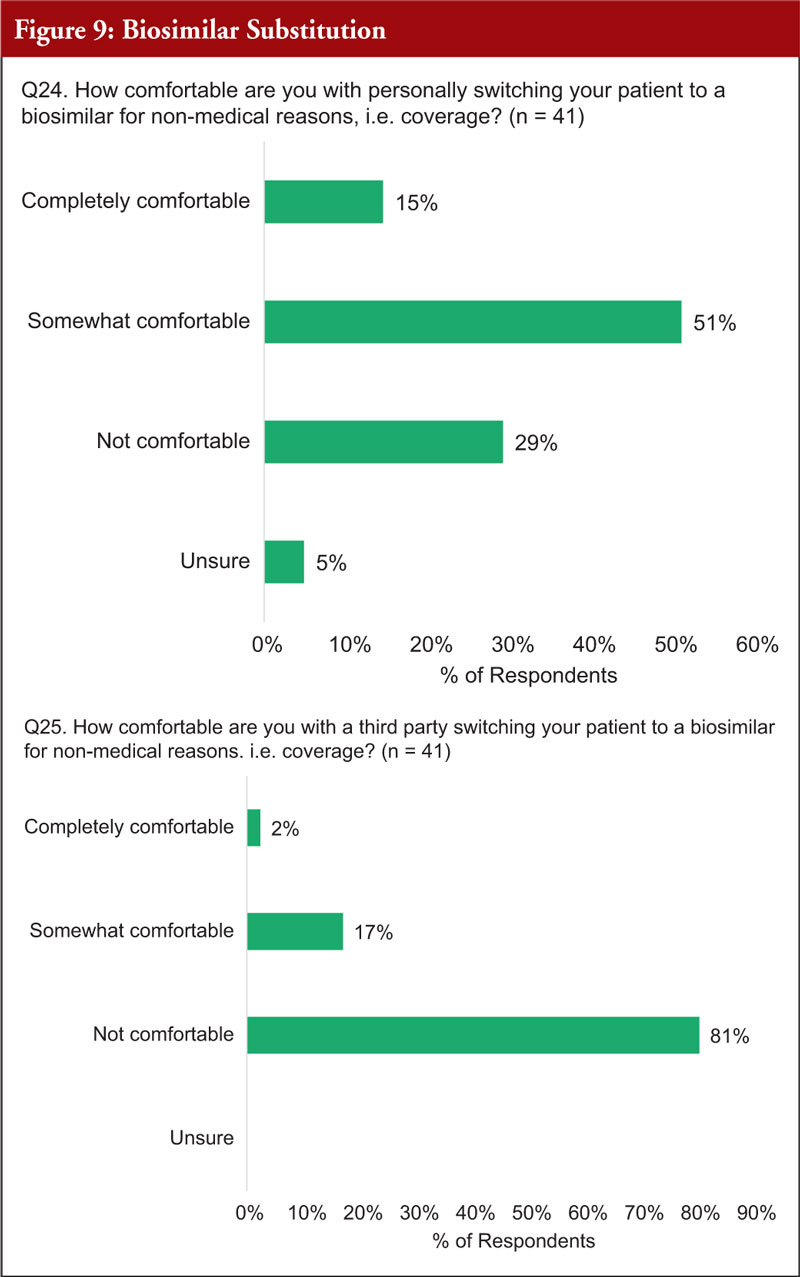
- Their comfort levels: a) when switching patients to a biosimilar for non-medical reasons, i.e. coverage; or b) with a third-party switching of a patient to a biosimilar for non-medical reasons, i.e. coverage.
- If a patient’s treatment gains were risked by switching to a biosimilar, would they be supportive of a patient’s right to choose the appropriate treatment for their individual circumstance?
- Their main concern about non-medical switching to a biosimilar.
- The importance of a) government tenders for biosimilars to be awarded to multiple suppliers; and b) factors besides price to be taken into account in national tender offers.
- Whether scenario a or b would be better for patients: a) is when multiple products, including innovator and biosimilars are reimbursed, and biosimilars may be encouraged for new patients with no automatic substitution permitted; and b) is when only government chosen biosimilars are reimbursed and new patients must be prescribed this and current patients forced to switch.
All data refer only to those who completed the survey. All data were analysed in MS Excel and checked manually.
Results
Identification and naming of biological products during use and reporting of adverse drug events
When carrying out the survey, participants were first given two explanatory texts to examine. These were given immediately preceding Question 7 (and 8):
- Biological medicines are therapeutic proteins produced using living cells. The active substances of biological medicines are larger and more complex than those of non-biological medicines. A biosimilar medicine is a biological medicine that is developed to be similar to an existing biological medicine (the ‘reference product’). Biosimilars are not the same as generics, which have simpler chemical structures and are considered to be identical to their reference medicines.
- In Canada biologicals and biosimilars are approved nationally by Health Canada under the New Drug Submission pathway. As a result of patent expiry on the originator products, biosimilars are increasingly becoming available in Canada. Unique to Canada, the patient support program (PSP) for a biological is paid for by the manufacturer and a change in biological medications means a change in PSP if the manufacturer is different.
The question considered whether or not prescribers identify biological or biosimilar products by their product/brand name or their non-proprietary /generic name, 80% said they used the brand name and 20% the non-proprietary. Regarding the reporting of adverse events, 78 % said they use the product/brand name, 20% use the non-proprietary name, and 2% use the Drug Identification Number (DIN) number.
When asked to consider how confident they were in the Canadian pharmacovigilance system’s ability to accurately identify the specific product, at the brand-name level, that might be responsible for an adverse drug reaction, 39% of participants were highly confident, 56% somewhat confident and 5% not confident.
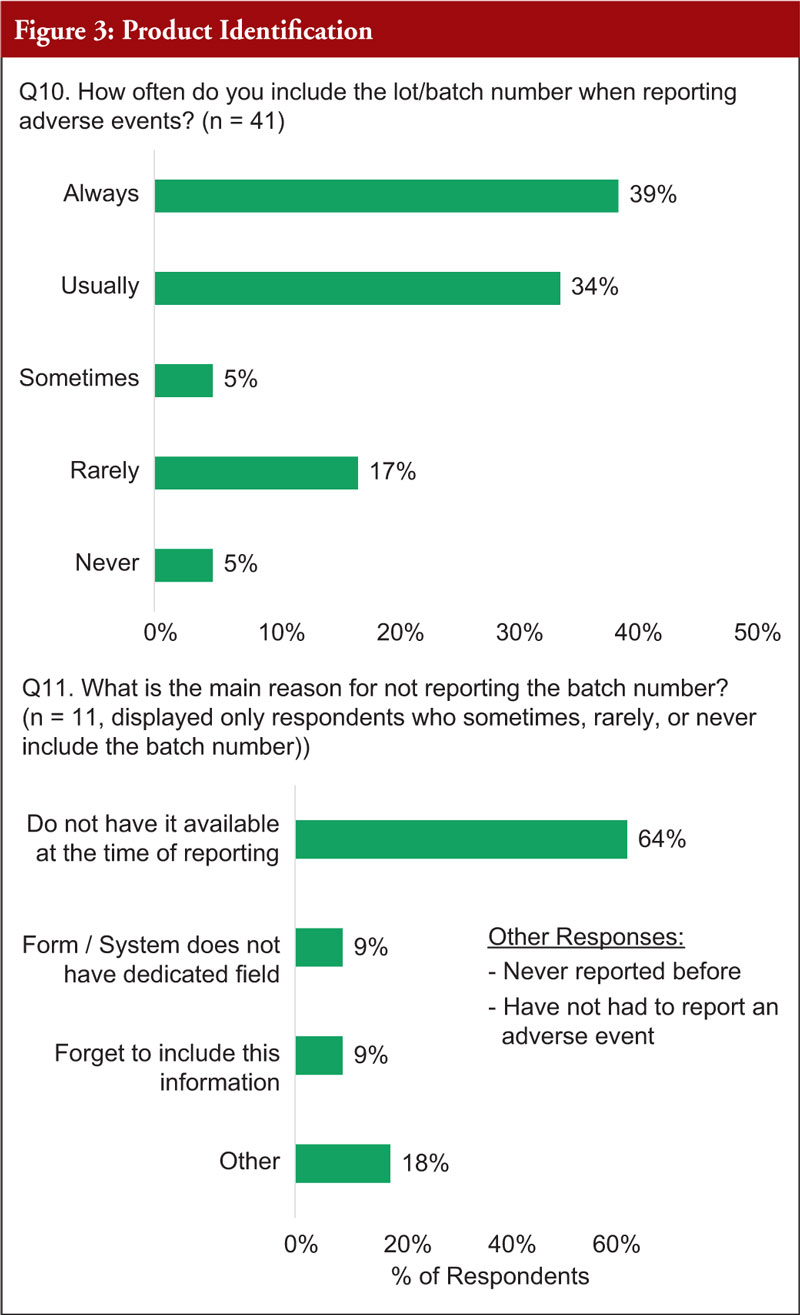
When asked whether they include the lot/batch number when recording adverse drug reactions, 39% of respondents said they always did this, 34% said they usually did, and 27% said this was done sometimes, rarely or never. Of the (11) respondents who said they sometimes, rarely or never recorded the lot/batch number, 64% said this was because they did not have it available at the time of reporting, 9% said the system/form does not have a dedicated field for this, 9% said they forget to include this information and 18% had other reasons, which include, that they have not yet had to report adverse drug reactions, see Figure 3.
Again, participants were first given two explanatory texts to examine. These were given immediately preceding Question 12.
- In 2015, the World Health Organization’s International Nonproprietary Names (INN) Programme proposed that a distinguishing suffix be appended to all biological medicines, including biosimilars, that share an INN to clearly differentiate them from each other and improve global pharmacovigilance. Health Canada was an early supporter of this proposal; and has indicated it would harmonize with the World Health Organization (WHO) if this system were made available.
- Health Canada has also held talks about harmonizing nomenclature with the US, which uses a suffix system similar to that proposed by WHO. Health Canada currently relies on self-reporting of brand name and DIN to differentiate similar products from one another.
Then, when asked if they would support Health Canada harmonizing internationally by adopting a distinct suffix system, the majority said they would support this (88%).
Prescribing biologicals: cost, switching, patient support programs and patient education
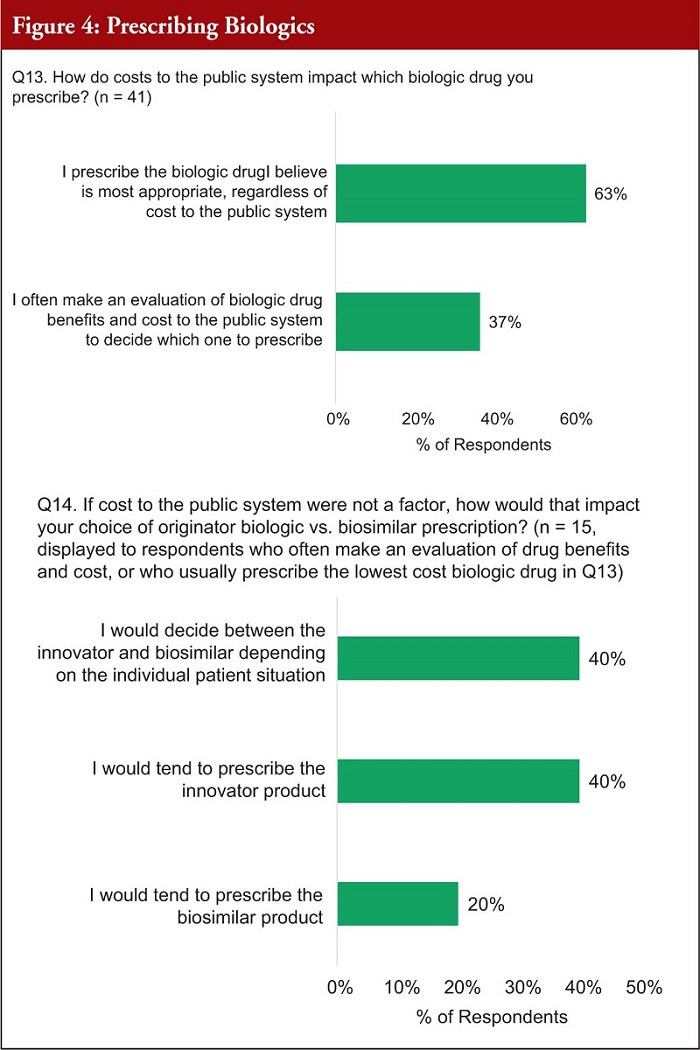
When asked about the cost of prescribing biologicals, 63% of respondents said they prescribe the biological drug they think is most appropriate regardless of cost, and 37% said they make an evaluation of the biological drug benefits and cost to the public system when prescribing. If cost was not a factor, of the (15) respondents who make an evaluation based on the cost of the product, 40% said they would decide between the innovator and biosimilar based on the individual situation, whereas 40% would prescribe the innovator, with 20% tending to prescribe the biosimilar, see Figure 4.
When asked about comfort levels when prescribing a biosimilar to a treatment naïve patient, 83% said they were very or somewhat comfortable and 17% were somewhat or very uncomfortable with this. When asked about switching a stable patient to a biosimilar, 62% said they were very or somewhat comfortable and 39% were somewhat or very uncomfortable with this, see Figure 5.
When asked if the quality of a biological’s PSP has an influence on which biological is prescribed, 53% of respondents said it has a moderate or significant influence and 46% of respondents said it had minimal or no influence, see Figure 6.

When asked about the importance of patient education on biosimilars prior to switching a patient to a biosimilar, 44% of respondents said it is critical or very important, 42% said it was somewhat important and 14% said it was slightly important or not important.
Prescribing biosimilars and substitution
Again, participants were first given two explanatory texts to examine. These were given immediately preceding Question 19 .
- Health Canada has stated, biosimilars are not ‘generic biologicals’ … authorization of a biosimilar is not a declaration of pharmaceutical equivalence, bioequivalence or clinical equivalence to the reference biological drug. Health Canada Biosimilar Guidance Document, November 2019.
- In Canada, the term ‘interchangeability’ often refers to the ability for a patient to be changed from one drug to another equivalent drug, by a pharmacist, without the intervention of the prescriber who wrote the prescription. The authority to declare two products interchangeable rests with each province/territory according to its own rules and regulations.
When faced with a situation where substitution by a pharmacist is an option in their province, 88% of practitioners thought it was critically or very important for them to have the authority to designate a biological medicine as ‘DISPENSE AS WRITTEN’ or ‘DO NOT SUBSTITUTE’, see Figure 7.
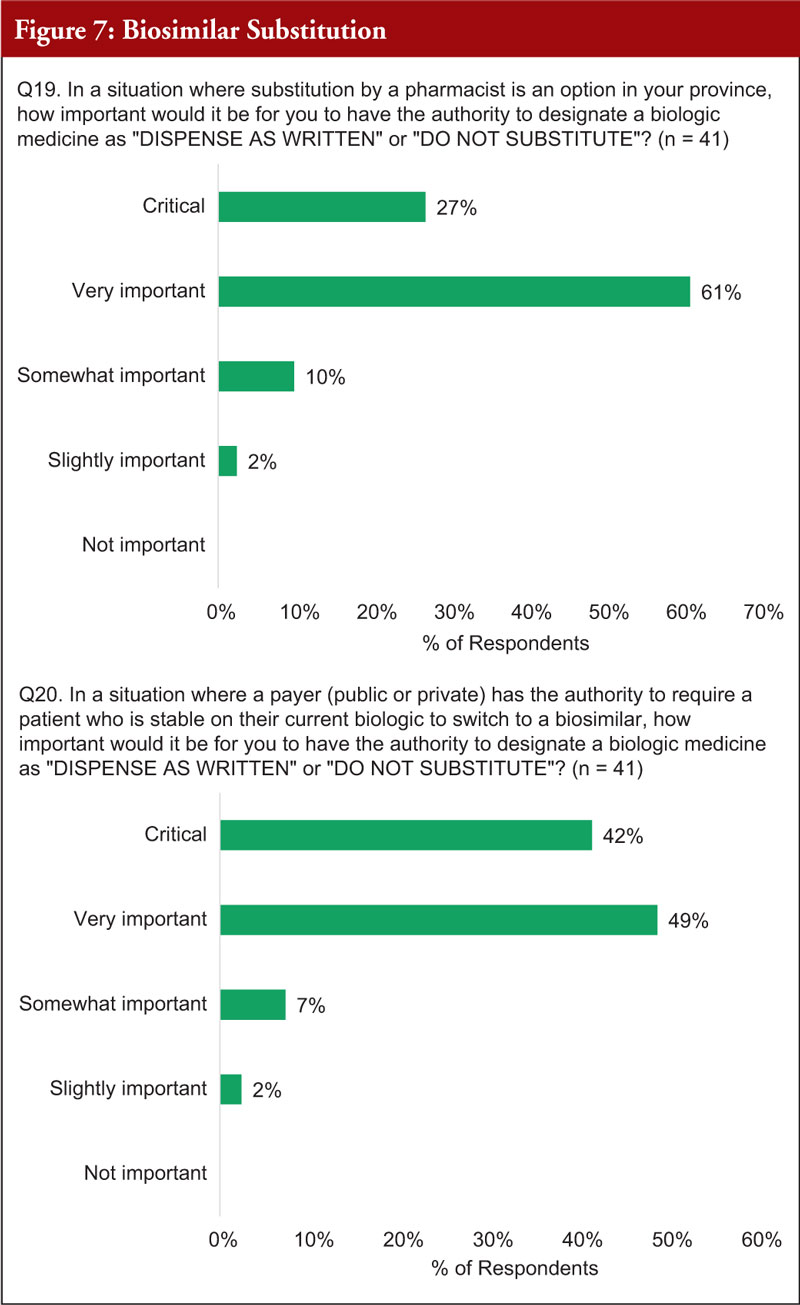
When faced with a situation where it is permissible for a payer (public or private) to require a patient who is stable on their current biological to switch to a biosimilar, 91% of practitioners thought it was critically or very important to have the authority to designate a biological medicine as ‘DISPENSE AS WRITTEN’ or ‘DO NOT SUBSTITUTE’, see Figure 7.
When asked about how important it would be for practitioners to be notified by the pharmacist that a patient has received a biological other than the one prescribed, if the patient was receiving chronic (repeated) treatment, 91% said it was critically or very important, see Figure 8.
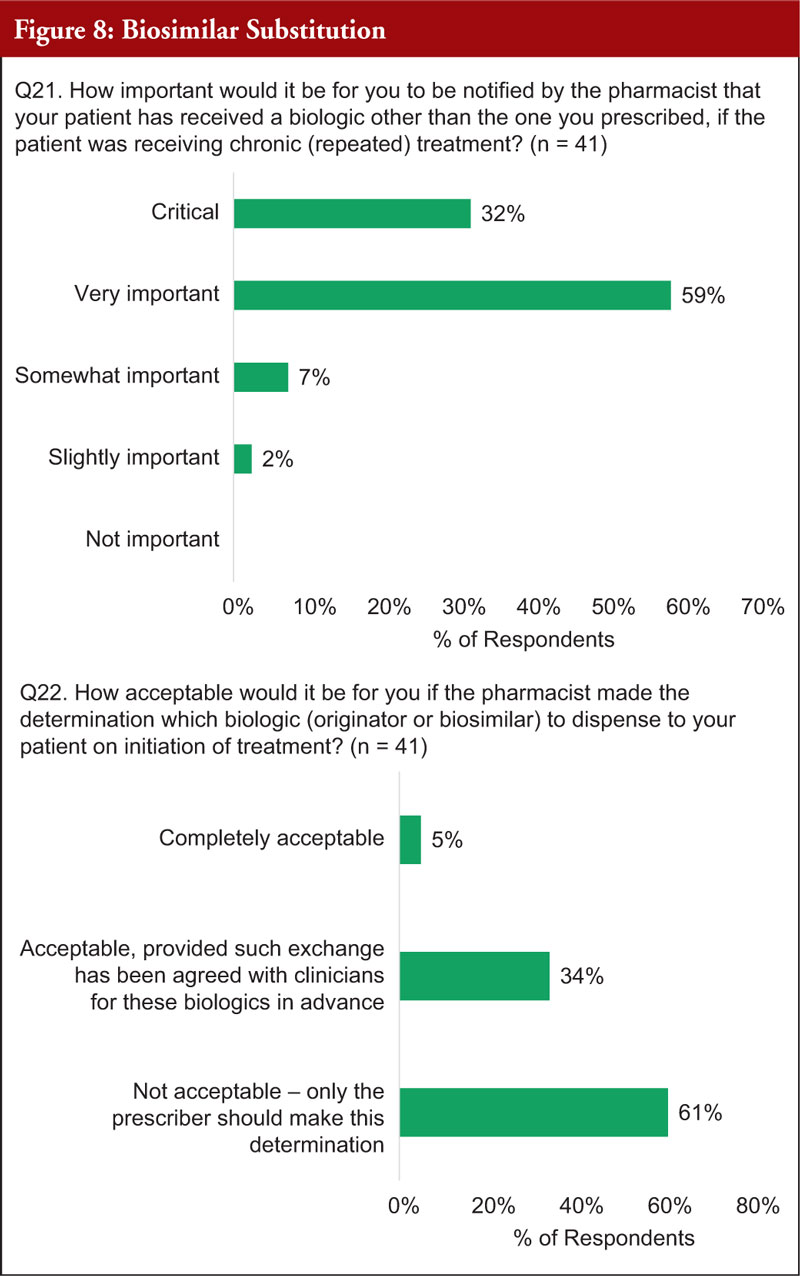
The majority (61%) thought it was not acceptable for a pharmacist to determine which biological (innovator or biosimilar) to dispense to a patient on initiation of treatment and the decision should be made by the practitioner. The minority (39%) thought it was either totally acceptable or acceptable, if agreed in advance, for a pharmacist to determine which biological (innovator or biosimilar) to dispense to a patient on initiation of treatment, see Figure 8.
The majority (90%) of practitioners stated that it was critically or very important for them to have the sole authority to decide, together with patients, the most suitable biological medicine for their disease.
Regarding personally switching patients to a biosimilar for non-medical reasons, i.e. cost or coverage, 66% of practitioners were very or somewhat comfortable with this idea, see Figure 9. Concerning third-party switching of a patient to a biosimilar for non-medical reasons, i.e. cost or coverage, 81% of practitioners stated they were not comfortable with this idea.
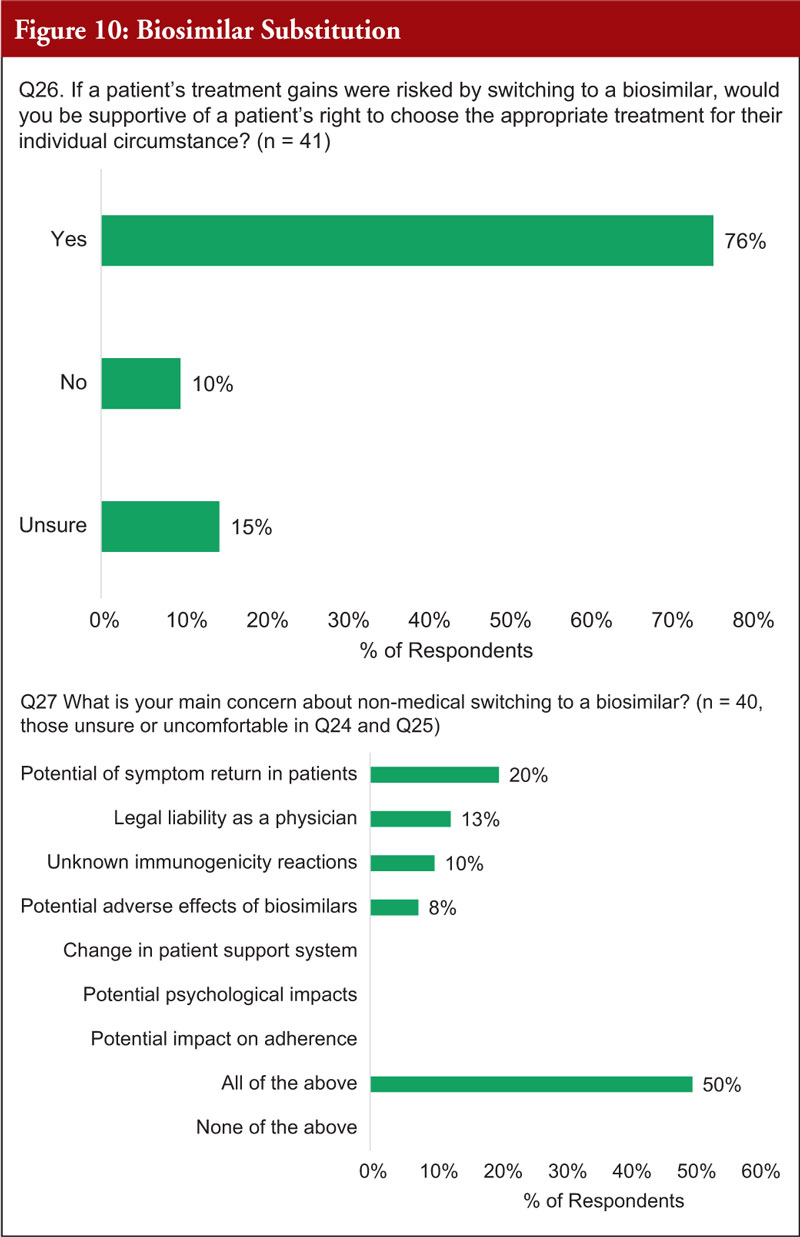
The majority (76%) said that if patient’s treatment gains were risked by switching to a biosimilar, they would be supportive of a patient’s right to choose the appropriate treatment for their individual circumstance.
When asked about their main concerns about non-medical switching to biosimilars, the top concerns were potential symptom return in patients (20%), legal liability as a physician (13%), unknown immunogenicity reactions (10%) and potential adverse effects of biosimilars (8%). However, the remaining 50% of practitioners responded ‘All of the above’ which also included, change in patient support system, potential psychological impacts, and potential impact of adherence, see Figure 10.
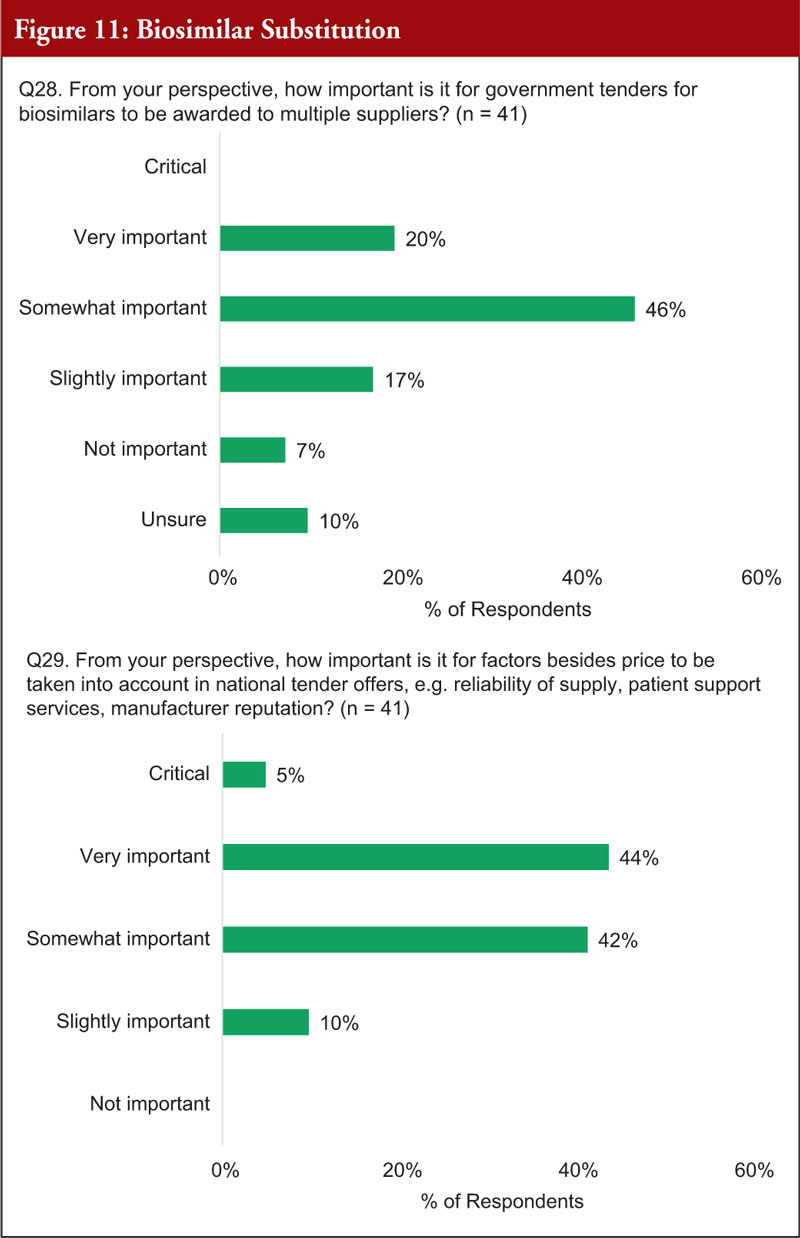
When asked about the importance of government tenders for biosimilars to be awarded to multiple suppliers, 66% said it was very or somewhat important. Regarding how important it is for factors besides price to be taken into account in national tender offers, e.g. reliability of supply, patient support services, manufacturer reputation, 91% said it was critical, very or somewhat important, see Figure 11.
Again, participants were first given two explanatory texts to examine. These were given immediately preceding Question 30.
- In nearly every Western European country, physicians are encouraged to prescribe lower-cost biosimilars to new patients, but ultimately retain the authority to choose between multiple products when prescribing – all of which will to be reimbursed by the payer. Automatic or forced substitution is strongly discouraged and cost savings are achieved through competition between multiple reimbursed products.
- In contrast, some Canadian provinces are adopting the approach used in Eastern Europe: all patients, both treatment-naïve and those who are stable on their current biological, will be switched to the preferred, government-chosen biosimilar in order to achieve cost savings.
Following this, the majority (78%) said that the system that would best serve the patients of their province would be one in which multiple products, including innovator and biosimilars, are reimbursed, biosimilars are encouraged for new patients and there is no automatic substitution. However, 15% said that they supported a system where only government-chosen biosimilars are reimbursed, new patients must be prescribed to this product and current patients are forced to switch.
Conclusion
The survey demonstrates information about Canadian ophthalmology physicians’ thoughts on the use of biosimilars for ocular use. Specifically, it reveals information about how these physicians record and identify biological/biosimilar drug products (product identification) and shows that the ophthalmologists are confident in the Canadian pharmacovigilance system’s ability to accurately identify the specific product, at the brand-name level, that might be responsible for an adverse drug reaction. It also highlights that, regarding prescribing biologic al s, most physicians are not influenced by the cost when prescribing biologicals and they are confident prescribing biosimilars and switching patients to biosimilars where appropriate. They also hold patient education and support programmes in high regard. Overall, physicians believe that, regarding switching (by pharmacists or payers), it is important that physicians have the authority to designate a biological medicine as ‘DISPENSE AS WRITTEN’ or ‘DO NOT SUBSTITUTE’ and they want to be informed when pharmacists dispense biologicals that differ to those prescribed. Overall, 90% of practitioners think they should have the sole authority to decide what biological is dispensed to patients and over 80% are not comfortable with third-party switching for non-medical reasons. The majority of practitioners said that the system that would best serve the patients of their province would be one in which multiple products, including innovator and biosimilars, are reimbursed, biosimilars are encouraged for new patients and there is no automatic substitution.
Funding sources
The survey study was funded by the Alliance for Safe Biologic Medicines (ASBM) and administered by Industry Standard Research, LLC.
The ASBM is an organization composed of diverse healthcare groups and individuals – from patients to physicians, innovative medical biotechnology companies and others – who are working together to ensure patient safety is at the forefront of the biosimilars policy discussion.
The activities of the ASBM are funded by its member partners who contribute to ASBM’s activities. Visit www.SafeBiologics.org for more information.
Authors
Michael S Reilly, Esq
Executive Director, Alliance for Safe Biologic Medicines, PO Box 3691, Arlington, VA 22203, USA
Jane Barratt, PhD
Secretary General, International Federation on Ageing, Suite G.238, 1 Bridgepoint Drive, Toronto, Ontario, M4M 2B5, Canada
Competing interests: Mr Michael S Reilly, Esq is the Executive Director and employed by Alliance for Safe Biologic Medicines. Mr Reilly served in the US Department of Health and Human Services from 2002 to 2008.
Dr Jane Barratt is the Secretary General, International Federation on Ageing and has no conflicts of interest. Unrestricted grants and sponsorship have been received in the field of vision health for more than a decade.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
1. GaBI Online – Generics and Biosimilars Initiative. Trends in biological drugs in Canada [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2023 Apr 25]. Available from: www.gabionline.net/reports/Trends-in-biological-drugs-in-Canada
2. GaBI Online – Generics and Biosimilars Initiative. Biosimilars approved in Canada [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2023 Apr 25]. Available from: www.gabionline.net/biosimilars/general/biosimilars-approved-in-canada
3. GaBI Online – Generics and Biosimilars Initiative. Canada approves five biosimilars in last seven months [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2023 Apr 25]. Available from: www.gabionline.net/biosimilars/news/canada-approves-five-biosimilars-in-last-seven-months
4. GaBI Online – Generics and Biosimilars Initiative. Canada approves ranibizumab biosimilar Byooviz [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2023 Apr 25]. Available from: www.gabionline.net/biosimilars/news/canada-approves-ranibizumab-biosimilar-byooviz
5. GaBI Online – Generics and Biosimilars Initiative. ‘Similar biologics’ approved and marketed in India [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2023 Apr 25]. Available from: www.gabionline.net/biosimilars/general/Similar-biologics-approved-and-marketed-in-India
6. Sharma A, Kuppermann BD, Loewenstein A. The future of biosimilars and biobetters in ophthalmology. touchREVIEWS in Ophthalmology. 2022;16(1):6–7.
7. Biogen. FDA Approves Samsung Bioepis and Biogen’s BYOOVIZTM (SB11), LUCENTIS® Biosimilar (ranibizumab-nuna) [homepage on the Internet]. [cited 2023 Apr 25]. Available from: https://investors.biogen.com/news-releases/news- release-details/fda-approves-samsung-bioepis-and-biogens-byooviztm-sb11
8. Ranibizumab biosimilar (Byooviz) gains EU marketing authorization. Am J Manag Care. 2021 Aug 30. https://www.centerforbiosimilars.com/view/samsung-bioepis-byooviz-gains-ema-marketing-authorization.
9. GaBI Online – Generics and Biosimilars Initiative. Biosimilars of ranibizumab [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2023 Apr 25]. Available from: www.gabionline.net/biosimilars/general/Biosimilars-of-ranibizumab
10. Sharma A, Parachuri N, Kumar N, Bandello F, Kuppermann BD. Biosimilar anti-VEGF-yardsticks to ensure biosimilarity. Eye. 2023;37(4-5).
11. Hariprasad SM, Gale RP, Weng CY, Ebbers HC, Rezk MF, Tadayoni R. An Introduction to biosimilars for the treatment of retinal diseases: a narrative review. Ophthalmol Ther. 2022;11(3):959-82.
12. European Medicines Agency. Zaltrap summary of product characteristics. 2017 [homepage on the Internet]. [cited 2023 Apr 25]. Available from: https://www.ema.europa.eu/en/documents/product-information/zaltrap-epar-product-information_en.pdf
13. Daien V, Nguyen V, Essex RW, Morlet N, Barthelmes D, Gillies MC; Fight Retinal Blindness! Study Group . Incidence and outcomes of infectious and noninfectious endophthalmitis after intravitreal injections for age-related macular degeneration. Ophthalmology. 2018;125(1):66-74.
14. Goldberg RA, Flynn HW Jr, Isom RF, Miller D, Gonzalez S. An outbreak of streptococcus endophthalmitis after intravitreal injection of bevacizumab. Am J Ophthalmol. 2012;153(2):204-8.e1.
15. Ricci F, Calabrese A, De Felici C, Missiroli F, Pileri M, Regine F. A cluster of presumed, noninfectious endophthalmitis after intravitreal injection of bevacizumab: long-term follow-up. Digit J Ophthalmol. 2016;22(2):41-5.
16. VanderBeek BL, Bonaffini SG, Ma L. Association of compounded bevacizumab with postinjection endophthalmitis. JAMA Ophthalmol. 2015;133(10):1159-64.
17. American Academy of Ophthalmology. Position Statement. Use of biosimilars in ophthalmic practice. 2022 Jan [homepage on the Internet]. [cited 2023 Apr 25]. Available from: https://www.aao.org/clinical-statement/use-of-biosimilars-in-ophthalmic-practice
18. GaBI Online – Generics and Biosimilars Initiative. American Academy of Ophthalmology biosimilars position statement published [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2023 Apr 25]. Available from: www.gabionline.net/biosimilars/general/american-academy-of-ophthalmology-biosimilars-position-statement-published
19. Sharma A, Holz FG, Regillo CD, Freund KB, Sarraf D, Khanani AM, et al; International Retina Biosimilar Study Group (Inter BIOS Group). Biosimilars for retinal diseases: United States – Europe awareness survey (BIO-User – survey). Expert Opin Biol Ther. 2023:1-9. doi:10.1080/14712598.2023.2176218
20. GaBI Online – Generics and Biosimilars Initiative. Concerns over Canada’s New Brunswick transition to biosimilars [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2023 Apr 25]. Available from: www.gabionline.net/biosimilars/general/concerns-over-canada-s-new-brunswick-transition-to-biosimilars
21. A survey of Australian prescribers’ views on the naming and substitution of biologicals. Generics and Biosimilars Initiative Journal (GaBI Journal). 2017;6(3):107-13. doi: 10.5639/gabij.2017.0603.022
22. Dolinar RO, Reilly MS. Biosimilars naming, label transparency and authority of choice – survey findings among European physicians. Generics and Biosimilars Initiative Journal (GaBI Journal). 2014;3(2):58-62. doi: 10.5639/gabij.2014.0302.018
23. Feldman MA, Reilly MS. European prescribers’ attitudes and beliefs on biologicals prescribing and automatic substitution. Generics and Biosimilars Initiative Journal (GaBI Journal). 2020;9(3):116-24. doi:10.5639/gabij.2020.0903.020
24. Reilly MS, Gewanter HL. Prescribing practices for biosimilars: questionnaire survey findings from physicians in Argentina, Brazil, Colombia and Mexico. Generics and Biosimilars Initiative Journal (GaBI Journal). 2015;4(4):161-6. doi: 10.5639/gabij.2015.0404.036
25. Gewanter HL, Reilly MS. Naming and labelling of biologicals – a survey of US physicians’ perspectives. Generics and Biosimilars Initiative Journal (GaBI Journal). 2017;6(1):7-12. doi: 10.5639/gabij.2017.0601.003
26. Schneider PJ, Reilly MS. Naming and labelling of biologicals – the perspective of hospital and retail pharmacists. Generics and Biosimilars Initiative Journal (GaBI Journal). 2016;5(4):151-5. doi:10.5639/gabij.2016.0504.040
27. McKibbin RD, Reilly MS. US prescribers’ attitudes and perceptions about biosimilars. Generics and Biosimilars Initiative Journal (GaBI Journal). 2022;11(3):96-103. doi:10.5639/gabij.2022.1103.016
|
Author for correspondence: Michael S Reilly, Esq, Executive Director, Alliance for Safe Biologic Medicines, PO Box 3691, Arlington, VA 22203, USA |
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2023 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.


