An assessment of trends in the Iranian pharmaceutical market following domestic production of selected medications (2007‒2017) and new considerations for health policymakers
Published on 2021/01/07
Generics and Biosimilars Initiative Journal (GaBI Journal). 2021;10(1):33-43.
Author byline as per print journal:
Marzieh Zargaran1, PharmD, PhD Candidate; Abdol Majid Cheraghali 2,3, PharmD, PhD; Fatemeh Soleymani1,2, PharmD, MPH, PhD; Rajabali Daroudi4, BSc, MSc, PhD; Ali Akbari Sari4, MD, PhD; Professor Shekoufeh Nikfar1,2, PharmD, MPH, PhD
|
Background: Enacting national policies which empower the local production of medications is a promising way to improve the accessibility and affordability of medications, but this can also have unintended consequences. A number of such policies have been adopted by the Iranian government. This study was designed to examine the changes in the consumption of a number of selected pharmaceuticals which occurred in the years after these selected products began to be domestically produced. The implications of these changes were then evaluated for their potential to suggest possible policy changes. |
Submitted: 28 February 2020; Revised: 29 December 2020; Accepted: 2 January 2021; Published online first: 15 January 2021
Introduction/Background
The domestic production of medications in developing countries can motivate and empower pharmaceutical industries and can enhance the accessibility of medications [1]. After the 1979 Islamic revolution in Iran, a comprehensive generic drug-based system was developed through the Iranian national drug policy (NDP), to promote affordable access to various types of medications [2]. To support the domestic production of generic medications and vaccines, the creation of a national pharmaceutical industry and national self-sufficiency in vaccine production were key aspects of the policy [3].
With 60 years’ experience in domestic medication production, the Iranian government has placed great emphasis on empowering the domestic pharmaceutical industry in recent decades [4, 5]. According to clause 28 of the health regulations laid out in the sixth Iranian development plan, at least 10% of National Development Fund resources have been deposited into domestic banks to promote the infrastructure of the health system, including that required for the production of pharmaceutical materials and products. In addition, to accomplish self-sufficiency of the pharmaceutical industry, clause 29 of the document obliges the Iranian Ministry of Health (MoH) to support and endorse domestic pharmaceutical plants.
A number of policies have been implemented to encourage Iranian pharmaceutical manufactures to develop their production capacity. High tariffs are imposed on imported medications, and in many cases imported medications are substituted with similar domestically produced alternatives present on the national reimbursement list (a list of medicinal products which are reimbursed through public health insurance), both of these policies reduce or prevent the import of certain foreign medications [2, 5].
Between 2010 and 2017, there was a significant increase (from 89 to 167) in the number of companies engaged in the production of pharmaceuticals in Iran. In addition, the number of companies importing pharmaceuticals during this time reduced from 207 to 93. There was also 1,213% growth in the price of the domestic pharmaceutical products between 1997 and 2010 [6]. However, it is noted that, despite the efforts of the Iranian government to support their national pharmaceutical industry, it is not yet comprehensively self-sufficient [2]. Due to the administration of the Health Sector Evolution Plan (HSEP) in 2014, and new approaches of MoH to support the national pharmaceutical industry, the annual pharmaceutical importation cost reduced from US$1 billion in 2013 to US$450 in 2014 [7].
Improvements in access to domestically produced pharmaceutical preparations can lead to additional changes in consumption patterns in some cases. The lower prices and greater affordability of domestically produced medications increases their availability and accessibility which can have some unintended consequences, such as their inappropriate and irrational consumption.
As such, comprehensive investigations on the management of national production and importation of pharmaceutical sciences are required. Identifying patterns of change in the consumption of medications associated with improvements in national pharmaceutical production will reveal future trends in the pharmaceutical market and help inform the decisions of policymakers.
This paper provides a 10-year overview of medication sales in terms of volume and value of imported medications after the development of domestic production lines in Iran. The main aim is to conduct a study to assess the trends in medication consumption after the initiation of domestic production. It also hopes to shed light on the unintended consequences of increased accessibility and affordability of medications brought about by increased domestic production, to help health policymakers in their future decision-making.
Finally, this review also aims to investigate the price of different selected medications.
Methods
Comprehensive literature review
A literature review was conducted to determine the best methods to assess the trends associated with domestically produced medications and relevant policies. ISI/Web of Science, PubMed/MEDLINE, Scopus, Google Scholar, as well as Iranian databases such as Irandoc, Scientific Information Database (SID), Magiran and the grey literature, were used to find studies, both in English and Persian, that contained the following Medical Subject Headings (MeSH) keywords: local production, pharmaceutical market trends, pharmaceutical industry, health policy, and pharmaceutical policy. The publications found were not constrained to a specific time period.
Medication selection
The method used to select the medications to be investigated was approved by Iranian Food and Drug Administration (IFDA) experts. This used data from Iranian pharmaceutical statistical datasheets which contain pharmaceutical sale statistics collected by IFDA from lists published annually by medication distribution companies. The sales volume and sales value of medications are reported in these data sheets and this is the most reliable data on medication consumption estimations in Iran. However, due to changes in IFDA policy, these datasheets are only available up to and including 2017. It is thought that new statistical datasheets will become available in the future.
In this study, pharmaceutical statistical datasheets between 2007 and 2017 were employed to find medications meeting the following requirements:
During the 10-year time period, they must have had a minimum of three years import history, followed by a minimum of two years of domestic Iranian production.
Figure 1 demonstrates the selection process and the sale history of 277 medications in the available statistical datasheets during the specified time period. For more than 80% of the medications, national pharmaceutical companies were able to domestically produce those which had been previously imported within three years of their introduction to the Iranian market. In addition, despite some medications being available in different strengths and dosage forms, each strength and dosage form of a particular medication were considered together.
The two-year period of domestic production was selected to ensure adequate follow up could be pursued and to ensure good comparisons between imported and domestic products could be made.

Consumption data collection
Data from the IFDA pharmaceutical statistical datasheets on the annual sales volume and value of the medications identified for study, was investigated. Although, the sales volume and value of both imported and domestically produced medications were scrutinized separately, the overall consumption trend of each medication was also investigated. At this stage, 108 graphs were analysed to determine the exact pattern of changes within the selected time period.
Price data collection
The price of pharmaceutical preparations is defined by the IFDA pricing committee and data on this is available on the IFDA website for free [8], however, the price of some preparations was not found which led to their exclusion from the study. In addition, due to the existence of various medication strengths, the price of each strength was separately reviewed. Thirteen medications were reviewed between 2014–2017 and the prices were calculated through converting Iranian Rials to USD in each respective year. Rial/USD conversion rate varied in successive years. All the exchange rates were obtained from the Central Bank of Iran, which was selected as the most reliable reference [9].
Inter-rate reliability was evaluated through checking the data by three members of the research team (for sales and price data) and the staff of IFDA (for price data).
Results
Literature review findings
The findings of the literature review indicate that there is no applicable method to appraise the trends of domestic Iranian pharmaceutical production that is in accordance with IFDA policies frameworks.
Consumption data analysis
During the 10-year period, only 28 of the 3,252 reviewed medications, that were either imported or domestically produced, were identified as eligible for inclusion in this study; having at least three years import history followed by a minimum of two years of domestic production. Considering all the strengths of each dosage form of the selected medications, a total of 57 preparations were scrutinized. The sales volume and value of these preparations in the respective years demonstrated various patterns of change in consumption of the imported medications after initiation of domestic production. Medications with similar changes in consumption pattern were categorized in separate groups.
Findings of this study revealed six patterns of change in consumption of the domestically produced medications which had been previously imported:
-
- Pattern 1: Increased sales of domestically produced medications along with an elimination of imported products.
- Pattern 2: Increased sales of domestically produced medications along with a reduction in the sales of imported products.
- Pattern 3: Increased sales of both domestically produced and imported medications, with more domestically produced medications being sold (and consumed) than those that were imported.
- Pattern 4: Increased sales of both domestically produced and imported medications, with more imported medications being sold (and consumed) than those that were domestically produced.
- Pattern 5: Reduced sales of domestically produced medications along with an increase in the sales of imported products.
- Pattern 6: Reduced sales of domestically produced medications along with a reduction in the sales of imported products.
Table 1 contains the 28 selected medications and their patterns of change during the time period of the investigation. The results show that medications of the same category can have various patterns of change.
According to IFDA reports, there was no unapproved importation, and all the imported medications were registered in the pharmaceutical statistical datasheets.

Price data analysis
Thirteen medications were reviewed between 2010 and 2014. Documents showed that after 2014, the registered prices of the selected medications have fluctuated less than the previous years, and in most of the cases the prices in Rial did not vary. Given the annual reduction of the exchange rate in recent years with respect to the Iranian Rial and USD, the price of medications in USD exhibited a downward trend.
Figures 2 and 3 present the prices of the domestically produced and imported medications in USD.


Discussion
Background
After resolution 61.21 of the World Health Assembly (WHA) was drawn up in 2008, many policies aiming to improve the domestic production of medications and to promote innovation and improvement in drug accessibility were designed in developing countries [10]. The aim of achieving self-sufficiency in pharmaceuticals production is considered one of the most important health system policies [11].
Recently, empowering domestic production of medications through policy implementation has also been occurring in low/middle income countries. The development of national pharmaceutical industries that produce generic drug products leads to lower prices, greater affordability and increased availability of medications [12]. This is seen in China, where domestic production of pharmaceutical products has been promoted through regulatory processes that are designed to facilitate the appraisal of new domestically produced medications [13]. Indian incentive policies have also dramatically affected the emergence of a successful pharmaceutical manufacturing sector. These include the establishment of Special Economic Zones (SEZs), modification of taxation system and price control [14]. In addition, developing countries have created some reforms to help implement self-sufficiency in pharmaceutical production, these include investment in developmental research and improvement of scientific capabilities [15].
The Iranian MoH has also adopted a domestic drug development approach to improve the availability and affordability of medications [16]. Since the implementation of HSEP in 2014, the Iranian government has supported the national production of medications through various strategies, such as imposing high tariffs on the imported medications, banning import of products similar to domestically produced preparations, supporting production of copy biopharmaceuticals produced by domestic industries, and substituting imported medications with similar domestically manufactured products present on the reimbursement lists [2, 5].
Medication consumption trends in Iran
In this study, products consisting of ingredients produced domestically and those containing imported ingredients to make the finished product are classified as domestically produced medications. It is important to note that there is no documented report that outlines how much pharmaceutical importation pertains to the importation of active pharmaceutical ingredients (APIs), rather than finished products. As such, the ratio of imported active ingredient to imported finished product has been considered.
When it comes to follow-on biologicals, all steps of the production of follow-on biologicals occurs in Iran. Cell line and cell culture processing are the first steps of the manufacturing of follow-on biologicals and the approval of domestically produced follow-on biologicals requires comparative experiments, as well as preclinical and clinical studies. Proving the similarity of physicochemical and biological characteristics of a reference product and the domestically produced preparation, is one of the most important steps of the follow-on biologicals product approval pathway [8].
Vaccines are domestically produced in Iran; however, they were excluded from this study as they are not under supervision of IFDA
Although there is no appropriate method for evaluating the trends in domestic production in the Iranian context, the data collecting/selecting method of this study has been approved by IFDA experts. Based on the designed method, only 28 preparations met the required criteria for further analysis.
This is the first study to characterize medication consumption trends in Iran. Further complementary studies to evaluate the assumptions made in this study may be required.
Medication consumption patterns
The findings of this study reveal various changes in the medication consumption patterns after the development of domestic production.
As shown in Table 1, medications classified in Patterns 1 and 2 were those with halted or reduced imports following the initiation of domestic production. Fourteen medications in different therapeutic categories exhibited these patterns, highlighting the domestically produced medications’ capability to reduce to the market share of imported medications.
However, the products that exhibit Pattern 3 indicate that in some cases, domestically produced medications fail to lower the market share of the imported products which leads to an increase in the total consumption rate of the medication regardless its origin (whether imported or domestically produced). The increase in the consumption rate of medications classified in Pattern 3 was rational in most cases. Here, non-communicable diseases have become more commonly diagnosed and treated in recent years, as such, related medications are also more commonly prescribed. Therefore, it is likely that increasing the total consumption rate now meets previously unmet demands.
In patterns 3 and 4 there is increased sales of domestically produced medications together with an increase in the sales of imported medications, however in Pattern 3 there are higher sales of domestically produced medications when compared to imported, and in Pattern 4 the sales of domestically produced medication are lower than imported. The difference between medications categorized in Patterns 3 and 4, is associated with the reduced market share of the imported medications following the domestic production of the medications in Pattern 4. However, the consumption of both imported and domestically manufactured medications significantly increased over the target years of the review.
Pattern 5 also addresses domestically produced medications which have failed to compete with imported products.
Only one of the selected medications belongs to Pattern 6, which indicates that despite the efforts of national industries to produce medications domestically, in some cases, reduction in the consumption rate occurred.
It is thought that determining the exact reasons that lead to the creation of the various medication consumption patterns can help Iranian health policymakers’ future decision-making. Understanding what lies behind the patterns will facilitate predicting the future path of other medications with similar charac-teristics.
These patterns demonstrate that the Iranian health system has been successfully supporting the domestic production of medications to increase accessibility and empower the domestic pharmaceutical industry. In 19 of the selected medications (67.8% of the medications), importation has been halted, reduced or increased (Pattern 3) after the empowering of national pharmaceutical industries which is indicative of the successful implementation of the policies supporting domestic production.
Sales value and volume of medications
Figure 4 highlights that there is an observed reduction in the sales value proportion of imported medications when compared to those that are domestically produced. Regression equations of the sales value trend charts showed similar gradients of the sales value proportions of imported and domestically produced medications when compared to total medication consumption, both when increasing and decreasing.
According to the regression equations of the trend lines shown in Figure 5, since 2014, there has been an increase in the sales volume of domestically produced medications compared with the total medication consumption (of those included in the study).
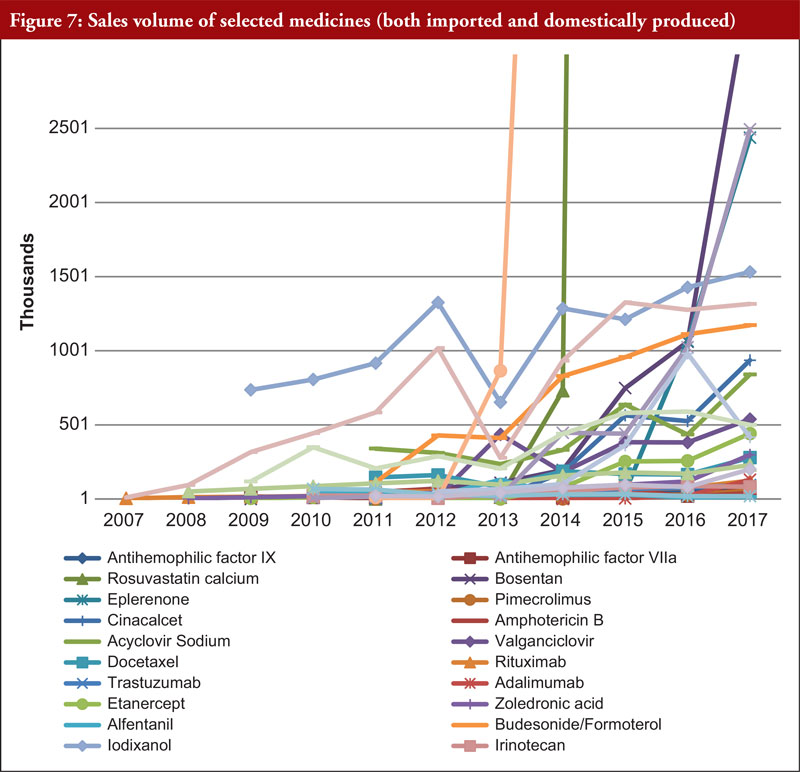
Figures 6 and 7 show a significant increase in the sales value and sales volume consumption of certain domestically produced medications after the increased production of national products. For example, after three years of rosuvastatin tablet imports, the importation of this medication has been discontinued. Additionally, in the second year of domestic production, the annual average growth rate (AAGR) of the sales value and volume was approximately 3,160 % and 5,063 %, respectively, indicating a significant increase in both the sales volume and sales value of domestically produced rosuvastatin tablets.
In some cases, the evolution of the annual market in terms of the total sales of each medication did not correspond with, and was greater than, the respective year’s population growth. Here, Iranian health policymakers face great challenges when it comes to explaining the multi-fold consumption of certain medications following the initiation of domestic production. Increased consumption of medications is associated with the irrational use of these medications in approved indications and the unreasonable use in off-label and unapproved indications, which may occur due to lower prices or greater availability of domestically produced medications. Moreover, physicians are allowed to prescribe the medications for off-label indications in accordance with their diagnosis, however off-label use is not included in reimbursement in Iran.
Increasing the consumption rate of some medications could potentially meet previously unmet demands brought about due to a lack of access to medicines; this assumption can be confirmed through further investigation.



Medication price
Of the 28 selected medicines with varieties of strength, only 13 medicines were reviewed in term of price, due to a lack of data on other medicines. The selection was not random or specific for a few medical classes. All the existing data on prices of medicine was reviewed.
Price analysis of the selected medications shows that since 2014, most of the selected domestically produced medications had a constant price in Rials. Due to the reduced exchange rate in recent years, domestic products have been presented at lower prices in USD. Comparisons of the trends in Figures 2 and 3 show that the price of the imported medications has increased more freely, therefore, importer companies experienced fewer price reductions when compared with manufacturers of the same products in Iran.
Based on the overall results of this investigation it is evident that, despite the government’s encouragement to support domestic manufacturers, in certain cases, domestically produced medications have failed to become viable competitors against imported products. According to Table 1, approximately 30% of the selected imported medications exceeded domestically produced medications in terms of volume over a period of at least two years.
Policy implications
In general, the domestic production of pharmaceuticals can be evaluated from two perspectives. On one hand, for industrial stakeholders, increasing the market share through development of products is very important for domestic production. On the other hand, increasing accessibility of medications is the most important factor for health policymakers [17].
In many countries, the domestic production of pharmaceutical preparations may increase medication consumption and increase money spent on the pharmaceutical industry. Encouraging approaches that aim to increase domestic production in developing countries is in accordance with national pharmaceutical policy goals [6]. However, studies have not yet shown a clear and strong relationship between the domestic production of pharmaceuticals and increased accessibility of medications [18].
Empowering the pharmaceutical industry to enhance the availability and affordability of pharmaceutical products has been the focus of the Iranian government. Supporting domestic employment, self-sufficiency and saving money on the foreign exchange are among other objectives of the Iranian health sector authorities.
This study has demonstrated that insistence upon strengthening domestic production policies for improvements of medication accessibility might be in contrary to the NDP goals, leading to the irrational use of medications and an increased financial burden on the health system.
Another controversial challenge is the lack of a viable and permanent alternative for domestically produced medications. Despite the high cost of these medications, domestically manufactured medications may not always be a proper substitute for imported products. In these cases, discontinuing the import of similar products can lead to reduced accessibility of desirable and adequate medication.
It should be mentioned that all domestically produced medicines in Iran pass specific qualification examinations prior to market release and as such, there are no perceived differences in quality of medicines that could influence specific product selection. However, it is often seen that patients tend to opt for branded originator medications.
In addition, the Iranian government requires detailed policies to prioritize the medications requiring investments for national pharmaceutical industry advances. In other words, the most appropriate medications need to be selected for domestic production as sustainable substitutes for imported ones.
This study is the first investigation of the consumption trends of pharmaceuticals in Iran and addresses the challenges encountered by the health system policymakers. The findings of this study suggest that further challenges in developing countries by the health policymakers need to be discussed.
Study limitations
The limitations of this study include the absence of similar research in this area due to the novelty of the topic, and inevitable errors in the data registration of statistical datasheets impacting on the outcomes of this study.
Pharmaceutical statistical datasheets based on distribution data are the only reliable references for estimating the sales of medications in Iran. Another important limitation of this research was that it assumed the medicine distribution data to be equal to medicine consumption or sales, although this may not be quite true. In addition, a lack of price data for some of the selected medications was the final limitation of this study.
Conclusion
From a health policy perspective, increasing domestic production of medications can have negative and unintended consequences. For example, increased accessibility following domestic production of medications may lead to greater unreasonable or irrational use of medications. Policymakers should be aware of such considerations and try to design reliable plans of medication selection for the domestic production of medications.
Acknowledgement
This research is part of a submitted doctoral dissertation in the faculty of pharmacy at Tehran University of Medical Sciences.
The authors are grateful to Dr Fatemeh Teymouri for her valuable assistance in some data collections.
The authors also thank Dr Marzieh Daniali for her ongoing collaboration in the English editing of this paper, and Ms Alice Rolandini Jensen, GaBI Journal editor, for English editing of the final version of this manuscript.
Competing interests: The authors have no conflicts of interest to declare.
Provenance and peer review: Not commissioned; externally peer reviewed
Authors
Marzieh Zargaran1, PharmD, PhD Candidate
Abdol Majid Cheraghali2,3, PharmD, PhD
Associate Professor Fatemeh Soleymani1,2, PharmD, MPH, PhD
Rajabali Daroudi4, BSc, MSc, PhD
Ali Akbari Sari4, MD, PhD
Professor Shekoufeh Nikfar1,2, PharmD, MPH, PhD
1Pharmacoeconomics and Pharmaceutical Administration Department, Faculty of Pharmacy, Tehran University of Medical Sciences, 16th Azar Street, Keshavarz Boulevard, 1417614411 Tehran, Iran
2Pharmaceutical Management and Economic Research Center, The Institute of Pharmaceutical Sciences (TIPS), Tehran University of Medical Sciences, Tehran, Iran
3Faculty of Pharmacy, BMS University, Tehran, Iran
4School of Public Health, Tehran University of Medical Sciences, Poorsina Avenue, Keshavarz Boulevard, 1417613151 Tehran, Iran
References
1. Kaplan W, Laing R. Health, Nutrition, and Population Family (HNP) of the World Bank’s Human Development Network (HNP Discussion Paper). Local production of pharmaceuticals: industrial policy and access to medicines. January 2005.
2. Nikfar S, Kebriaeezadeh A, Majdzadeh R, Abdollahi M. Monitoring of National Drug Policy (NDP) and its standardized indicators; conformity to decisions of the national drug selecting committee in Iran. BMC Int Health Hum Rights. 2005;5(1):5. doi:10.1186/1472-698x-5-5
3. Cheraghali AM, Nikfar S, Behmanesh Y, Rahimi V, Habibipour F, Tirdad R, et al. Evaluation of availability, accessibility and prescribing pattern of medicines in the Islamic Republic of Iran. East Mediterr Health J. 2004;10(3):406-15.
4. Lotfi K. Iran’s drug industry in the past 80 years (Part 1). Chem Dev. 2000;4:6-11.
5. Hashemi-Meshkini A. Making the public health and industrial objectives balanced; the big challenge of Iran’s Food and Drug Organization. Iran J Public Health. 2014;43(5):693-95.
6. Kebriaeezadeh A, Nassiri Koopaei N, Abdollahiasl A, Nikfar S, Mohamadi N. Trend analysis of the pharmaceutical market in Iran; 1997–2010; policy implications for developing countries. DARU J Pharm Sci. 2013;21(1):52. doi:10.1186/2008-2231-21-52
7. Dinarvand R. Significant reduction of drug imports to Iran with the implementation of the health system transformation plan. Government Information Database [homepage on the Internet]. [cited 2020 Dec 29]. Available from: http://dolat.ir/detail/288802.
8. Iran Food and Drug Administration [homepage on the Internet]. [cited 2020 Dec 29]. Available from: https://www.fda.gov.ir/en
9. Central Bank of Islamic Republic of Iran [homepage on the Internet]. [cited 2020 Dec 29]. Available from: https://www.cbi.ir
10. Sampath P, Mirza Z, Adachi K, et al. Local production for access to medical products: developing a framework to improve public health. World Health Organization. 2011.
11. United Nations Conference on Trade and Development. Local production of pharmaceuticals and related technology transfer in developing countries [homepage on the Internet]. [cited 2020 Dec 29]. Available from: https://unctad.org/system/files/official-document/diaepcb2011d7_en.pdf
12. World Health Organization. Local production and access to medicine in low- and middle-income countries. A literature review and critical analysis. 2011 [homepage on the Internet]. [cited 2020 Dec 29]. Available from: https://www.who.int/phi/publications/Local_Production_Literature_Review.pdf
13. World Health Organization. China policies to promote local production of pharmaceutical products and protect public health. 2017 [homepage on the Internet]. [cited 2020 Dec 29]. Available from: https://www.who.int/phi/publications/2081China020517.pdf?ua=1
14. World Health Organization. Indian policies to promote local production of pharmaceutical products and protect public health. 2017 [homepage on the Internet]. [cited 2020 Dec 29]. Available from: https://www.who.int/phi/publications/indian_policies_promote_local_production_pharm/en/
15. Siagian R, Thabrany H. Reforms in pharmaceuticals self-sufficiency in developing countries. Indian J Sci Tech. 2019;12(11):1-7.
16. Cheraghali AM. Trends in Iran pharmaceutical market. Iran J Pharm Res. 2017;16(1):1-7.
17. Gebre-Mariam T, Tahir K, Gebre-Amanuel S. Bringing industrial and health policies closer: reviving pharmaceutical production in Ethiopia. In: Mackintosh M, Banda G, Tibandebage P, Wamae W, editors. Making medicines in Africa. International Political Economy Series. Palgrave Macmillan, London. 2016; p. 65-84.
18. Kaplan WA, Ritz LS, Vitello M. Local production of medical technologies and its effect on access in low and middle income countries: a systematic review of the literature. South Med Rev. 2011;4(2):51-61.
|
Author for correspondence: Professor Shekoufeh Nikfar, PharmD, MPH, PhD, Pharmacoeconomics and Pharmaceutical Administration Department, Faculty of Pharmacy, Tehran University of Medical Sciences, Tehran, Iran |
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2021 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.


