Biosimilars: extrapolation of clinical use to other indications
Published on 2015/06/03
Generics and Biosimilars Initiative Journal (GaBI Journal). 2015;4(3):118-24.
|
Abstract: |
Submitted: 1 June 2015; Revised: 13 July 2015; Accepted: 13 July 2015; Published online first: 27 July 2015
Introduction
The extrapolation of biosimilar approval for all the clinical indications of the reference product can be justified based on scientific principles that begin with the precept that protein structure dictates function along with the totality of evidence. Biosimilars will be highly similar to the reference product in primary amino acid sequence, tertiary structure and biological activity as determined by rigorous analytical characterization in multiple assays. The biosimilar will have the same receptor or ligand binding and the same mechanism or mechanisms of action as the reference product. Clinical pharmacokinetic (PK) and pharmacodynamic (PD) studies and perhaps efficacy and safety data will confirm the biosimilarity determined at the analytical level. Thus, a biosimilar would have the same clinical performance as the reference for all approved indications.
Biosimilars should be approved for all the clinical indications of the reference product since extensive chemical, physical and biological comparisons demonstrate the same structure and function. There may be minor differences between a biosimilar and reference product that do not result in clinically meaningful differences. These differences are generally relatively small in comparison to product variants generated by post-licensing modifications. This is reflective of the nature of biologicals where no two batches of these products are the same. Likewise, the reference product undergoes changes when the manufacturing process is changed throughout its life cycle. Since the early 1990s, manufacturers have implemented manufacturing changes for protein therapeutics and monoclonal antibodies without the need for clinical efficacy and safety studies. The US Food and Drug Administration (FDA) and reference product sponsors have relied on the analytical characterization and non-clinical demonstration of biological activity as the most sensitive indicators of potential product changes. FDA has many years of experience in evaluation of potential product changes and their clinical impact and has developed guidance on comparability. Sponsors are able to implement process improvements or manufacturing site changes and demonstrate the new product is comparable to the previous product using analytical and non-clinical characterization. There is no change in labelling and the reference product retains all the approved indications. This approach for comparability is directly applicable to biosimilars with analytical characterization being the foundation in establishing biosimilarity.
The approval of a biosimilar for all clinical indications of the reference is also the key to retaining the linkage between the established clinical safety and efficacy of the reference and the projected clinical safety and efficacy of the biosimilar. Biosimilar approval depends on a demonstration that chemical, physical and biological parameters are highly similar to the reference product rather than a full clinical safety and efficacy programme in each indication. Any clinical studies conducted for biosimilars are limited and serve to confirm functional sameness and not to establish efficacy and safety de novo. Efficacy and safety have already been established with the reference product for all indications.
Extrapolation is essential to the concept of biosimilarity. Extrapolation requires an understanding that the biosimilar is sufficiently similar to the reference product using current assays that are highly sensitive and manufacturing process controls that are at least as good as that of the reference products. This ensures that the biosimilar will exert the same clinical effect across all diseases. Failure to extrapolate biosimilar use to all clinical indications of the reference product could create unnecessary confusion and undermine the concept of biosimilarity for physicians and patients. If a biosimilar cannot be approved for all clinical indications of the reference product one would question whether it is actually biosimilar. Extrapolation to all clinical indications is consistent with the globally recognized regulatory principle of comparability for originator/reference products as well as the approach for biosimilars in Europe and with generic drugs in the US.
Manufacture and characterization of therapeutic proteins and monoclonal antibodies
Most products being developed as biosimilars are recombinant proteins. Since 1982, when the first recombinant protein was approved, FDA has reviewed and approved numerous simple proteins, glycosylated proteins, fusion proteins and monoclonal antibodies. While each may be unique in its pharmacology, the methods used for production and purification of most recombinant proteins are similar in many aspects. Many of the host cells, fermentation procedures and purification steps are standard in the industry. The process starts when a human gene specific for a protein is inserted into a host cell to create a master cell bank. Proteins made in bacteria produce non-glycosylated proteins. Proteins made in yeast or mammalian cells, e.g. Chinese hamster ovary cells, can make glycosylated proteins. As the host cell grows and multiplies, it produces the human protein along with its own proteins. Purification is typically done through several chromatography steps. The final formulated protein product is highly purified (generally 95–98% pure).
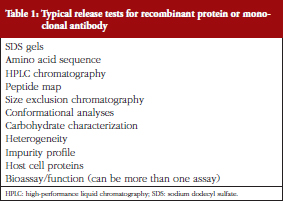
Biotech products are more like drugs in their characterization compared to other biologicals (vaccines, blood products). While proteins are larger and more complex than most drugs, they are not too complex to be characterized. In fact, FDA approved some very complex products such as enoxaparin and glatiramer acetate as generic drugs without a requirement for clinical efficacy data [1, 2]. FDA has approved hundreds of protein products over the past 30 years that are safe and effective. Analytical tests for proteins are more numerous and sophisticated than those for small-molecule drugs. Typical release tests for a recombinant protein or monoclonal antibody are shown in Table 1. These allow the rigorous assessment of proteins, product-related substances and process-related impurities.
Knowledge base from comparability studies is relevant to evaluation of biosimilars
Most protein therapeutics were originally regulated as biologicals in an era where the process defined the product. In the first decade of recombinant products, it was not certain if changes in manufacturing process would impact the product in such a way to affect clinical safety and efficacy. Therefore, most manufacturing changes required no new clinical data. Sponsors argued that biotech products could be characterized by their chemical, physical and biological attributes. In fact, analytical assessments were more likely to detect product changes than clinical studies because these are more precise, reproducible and more sensitive than clinical studies. There was concurrence from FDA and recognition that recombinant products were distinct from other biologicals in their ability to be characterized. This distinction was a factor in the transfer of review of most recombinant therapeutic proteins in FDA from the Center for Biologics Evaluation and Research (CBER) to the Center for Drug Evaluation and Research (CDER) in 2003.
Demonstration of comparability means that the product manufactured after the manufacturing change is analytically comparable to the product made before the manufacturing change. The expectation is that the product would have the same clinical safety and efficacy. Comparable does not imply identical as minor product changes are sometimes expected. As per the globally recognized regulatory guidance recognized by FDA and other health authorities [3] the standard for establishing comparability is high similarity, which is the same standard as for establishing biosimilarity. The effect of these minor differences is evaluated in in vitro biological activity and sometimes in PK studies. Only rarely, when more notable differences are observed, is clinical data required.
This concept is key for protein therapeutics since most products undergo changes in the manufacturing site, scale or process during the product life cycle. Manufacturers can and do change, e.g. the host cell, fermentation, purification process, manufacturing site; and still have a comparable product without the need to demonstrate safety and efficacy again. Analytical data is more sensitive in the ability to detect potential product changes than clinical trials.
FDA outlined their approach to comparability in the 1996 Guidance: demonstration of comparability of human biological products, including therapeutic biotechnology-derived products [4]. This guidance was released just prior to the approval of Biogen’s Avonex for multiple sclerosis, a hallmark case in comparability studies. After completion of phase III studies, there were internal disputes such that the Avonex master cell bank and product used during phase III were no longer available. Biogen developed a new master cell bank, new manufacturing process and at a new facility. Using analytical comparability studies and PK data, Biogen demonstrated that the new Avonex was comparable to the product used in phase III without the need for new clinical efficacy studies [5]. Avonex is a complex, glycosylated IFN-beta and minor glycosylation changes were noted, but FDA deemed the new product comparable to the investigational product and approved the new product without additional clinical efficacy trials. The use of analytical comparability studies has been possible because the nature of the proteins or monoclonal antibodies can be characterized by analytical methods and advances in analytical techniques allow for sensitive assessment of proteins.
The use of comparability studies has been recognized internationally with the implementation of the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) document Q5E: Comparability of biotechnological/biological products [3]. This approach to evaluation of potential product differences after manufacturing changes has served FDA, industry and patients. FDA has more than 20 years experience in evaluation of manufacturing changes, product changes and their potential impact on safety and efficacy. Manufacturing changes over time are a normal part of the biological product life cycle. Physicians are not notified or aware of manufacturing changes or comparability data. There is no change in labelling and the product retains all the approved clinical indications. There is inherent reliance on FDA to review the analytical data to determine comparability.
Characterization of biosimilars
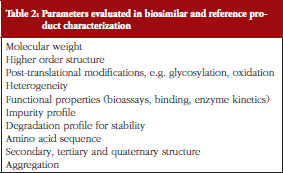
For biosimilars, side-by-side comparisons in multiple analytical assays would be expected. This was outlined in FDA Guidance for Industry: quality considerations in demonstrating biosimilarity to a reference protein product [6]. Different assays are often used to assess the same attribute in an orthogonal approach. Extensive, robust, physicochemical comparisons are made between the biosimilar and the reference, see Table 2 for the list of parameters typically assessed.
Biological activity relevant to the mechanism of action is compared in bioassays, binding assays to receptor or ligand, or possibly enzyme kinetics. Some bioassays may be more relevant than others. When possible, FDA recommends development of bioassays that are sensitive to changes in the functional activities of the product and these assays should be assessed for variability and reliability.
Newer analytical assays available today are more sensitive than those available when the reference product was approved. This is particularly true for characterization of carbohydrates, conformational studies and aggregates. For biosimilars, the site and type of carbohydrate linkage would typically be compared to reference product as well as quantitation of specific carbohydrates and ratios of various glycoforms. For any glycosylated protein the manufacturer would set specifications for major glycoforms and specific carbohydrates.
Conformational analyses are used to compare the three-dimensional structure and folding of the biosimilar and reference products. This analysis is extremely important because the conformational structure affects the functioning of the protein. Conformation is often assessed through circular dichroism, nuclear magnetic resonance, or possibly X-ray crystallography.
There is also more focus on assessment of aggregation today because of the association of aggregation with an increased risk of immunogenicity [7, 8]. With older reference products there may have been minimal attention on aggregation. Aggregates are often monitored by size exclusion chromatography, analytical ultra-centrifugation, light scattering, or field flow fractionation. Specifications are typically set for the level of aggregates and aggregation is followed on stability.
These are general approaches used in characterization of biosimilars. There is no single approach that is applicable to all proteins. There is a higher level of expectation for product characterization for all biotech products today, including biosimilars, than there was for the reference product when it was approved. Demonstration of biosimilarity involves application of this higher level of characterization to both the reference product and biosimilar, and demonstration that any differences observed do not adversely impact efficacy or safety. In addition to the extensive comparison to the reference product, biosimilars would undergo testing for each manufacturing batch after approval. Like all manufacturers, biosimilar sponsors must demonstrate consistency and control over the manufacturing process, comply with Good Manufacturing Practices, and undergo routine FDA inspections.
Biological products have more variability than drugs because they are produced from living organisms. This is especially true for glycosylated products where the ratio of glycoforms can vary from lot to lot and after a manufacturing change. However, there is some microheterogeneity observed even with simple proteins. The range of heterogeneity permitted is limited by specifications based on manufacturing history, which must be approved by FDA. Both the reference product and biosimilar will be held to the same standards.
The FDA requirements for biosimilarity, taken together with greater sensitivity of assays and advances in manufacturing controls, ensures that biosimilars will not have any greater variability than the reference product. Most biosimilars will be as close to the reference product chemically, structurally and biologically as the reference product is to itself from lot to lot. There is undue focus on the fact that biosimilar might be slightly different from the reference product. While this is true for biosimilars, we must also recognize that it applies to biologicals generally and thus, that the reference product is, of necessity, different from itself over time and from lot to lot [9].
For all of the comparisons between a biosimilar with the reference product the term used by FDA and others is ‘highly similar’ instead of the same. This distinction implies that there are differences between the biosimilar and reference product. While this may be true, the term can be misunderstood. Scientists wish to be accurate and because there are minor differences between two products or limitations of the assay we prefer the term highly similar. The notion that the reference product is unchanging over time is not accurate. The reference product is not identical after a manufacturing change or even from lot to lot. It would be highly similar to the previous product. Biosimilar will not have any clinically meaningful differences in safety or efficacy compared to the reference product. We should be cautious that the caveats of our terms do not overshadow the true meaning.
Extrapolation to other clinical indications for biosimilars
The scientific basis for comparability for biotechnology products can be extended to biosimilars. The assumption is that one can change the manufacturing process and still have the same product. With biosimilars, one is not re-establishing the safety and efficacy of the product. That has been established for the reference product. The goal is to demonstrate that the biosimilar is sufficiently similar to the reference product such that it will have no clinically meaningful differences. This is analogous to comparability studies after manufacturing changes in the reference product. FDA’s knowledge base on comparability studies and the impact of manufacturing changes is relevant in the review of biosimilars.
FDA provided guidance on extrapolation of approval across multiple clinical indications for biosimilars [10]. Extrapolation is justified based on similar mechanism of action, target/receptor interactions and molecular signalling; product structure interactions with the target or receptor; PK, expected toxicities and information based on mechanism of action. All of these are recommended for a biosimilar 351(k) applicationA. However, any differences in these factors can be addressed in the context of the totality of the evidence supporting a demonstration of biosimilarity. Thus, the totality of the evidence supersedes these other considerations.
It is a basic tenet of protein chemistry that structure dictates function. A biosimilar is designed to be highly similar to the reference product. Thus, the same structure should equate to the same function. Characterization of a biosimilar includes extensive analytical comparisons with the reference product using orthogonal methods to assess primary amino acid sequence, tertiary structure, post-translational modifications (primarily glycosylation), and assessment of any impurities [1]. In addition, biological activity is compared through in vitro and sometimes in vivo assays. This analytical comparison demonstrating that the biosimilar is highly similar to the reference product is the foundation of biosimilar development and approval. Thus, a biosimilar with highly similar structure, chemical, physical and biological attributes would be expected to produce the same pharmacology and thus highly similar safety and efficacy as the reference in every clinical indication.
The analytical characterization is easier for non-glycosylated proteins than it is for glycosylated proteins. Differences in glycosylation have the potential to affect bioactivity and possibly PK. However, characterization of carbohydrates has significantly improved in recent years. The quantification of specific sugars and the characterization of glycoform species are routine. The degree of carbohydrate characterization for glycoproteins is typically more extensive than what was available when the reference product was approved. As with comparability studies, differences between a biosimilar and reference product can be further analysed in in vitro and in vivo studies. The sponsor should determine if the differences affect the bioassay, binding, or other in vitro measures of biological function as well as PK. For example, any differences in glycosylation might be further assessed to determine if these differences have an impact on bioactivity or PK in comparison with the reference product. A biosimilar would be expected to demonstrate the highly similar bioactivity and PK as the reference product. If regulators determine that these tests are not adequate to confirm safety and efficacy, additional testing may be requested.
Another basic assumption that supports the extrapolation of a biosimilar to all clinical indications is that a biosimilar must have the same mechanism of action as the reference product (to the extent it is known). For most proteins, the mechanism of action depends upon the protein binding to a cell-associated receptor. While the binding of a protein to a receptor may occasionally cause distinct intracellular signalling reactions in different cell types, this receptor interaction is the same in all patients. Thus, the biosimilar would behave like the reference in all clinical indications. Examination of receptor binding is part of analytical characterization of biosimilars.
Mechanism of action is usually characterized by comparison of the biological activity of the biosimilar with that of the reference product. For some biosimilars there may be a need to examine several biological activities when the mechanism of action is pleiotropic or unknown. An advantage of biosimilar monoclonal antibodies is that the mechanism of action is usually well defined. Monoclonal antibodies are developed to a specific target. Thus, the comparison of a biosimilar monoclonal antibody to the reference product in the binding to the target antigen is the primary demonstration of similar mechanism of action.
FDA has stated that extrapolation to other clinical indications may depend on differences in expected toxicities for biosimilars. While biosimilars may have slightly different impurities than the reference product, it is important to remember that for most therapeutic proteins, any toxicity is due to the exaggerated pharmacology of the protein rather than as a result of impurities. The assessment of product related impurities, such as aggregates, which may be associated with increased immunogenicity, are much more rigorously monitored in today’s products than when the reference product was approved. A fundamental principle of biosimilar development is the reliance on the history of safety of the reference product and the known toxicities observed after many years of clinical use. We can also look to the use of biosimilars in Europe where biosimilars have been used for nearly 10 years and there have been no issues of safety unique to biosimilars [11–13]. In each clinical indication, a variety of biosimilars have demonstrated similar safety issues as the reference product, including in the extrapolated indications.
The extrapolation of biosimilars to all clinical indications of the reference product is also justified based on the experience following manufacturing changes made to protein therapeutics. Only rarely are any additional clinical studies required and if necessary would be conducted in a limited number of patients in a single indication. The ‘new’ product retains approval of all clinical indications of the ‘old’ product. The same principles would apply to biosimilars.
The comparability approach currently used by industry and FDA can be shown in several examples. Scientists followed three glycosylated proteins over time and demonstrated changes in darbepoetin alfa (Aranesp), rituximab (Rituxan) and etanercept (Enbrel) over time [9]. Darbepoetin alfa is a glycoprotein that stimulates red blood cells and is indicated for the treatment of anaemia due to chronic kidney disease for patients on dialysis and those not on dialysis [14]. Changes were noted for darbepoetin alfa (Aranesp) over time, with a higher sialylation rate (which affects PK) in batches expiring before April 2010 compared to batches expiring after September 2010. This corresponded with a major process change of Aranesp in 2008 approved by European Medicines Agency (EMA).
Rituximab (Rituxan) is a monoclonal antibody to CD20 antigen and is indicated for use in non-Hodgkin’s lymphoma, chronic lymphocytic leukaemia and rheumatoid arthritis when used with methotrexate for patients who failed anti-TNF therapy [15]. There were changes in glycosylation of rituximab noted in 2009–2010 (reduction in the basic variants, C-terminal lysine and N-terminal glutamine from 30–50% to 10%) [9]. A further change was also found in the amount of fucosylated glycans and G0 glycans with an increase in antibody dependent cellular cytotoxicity (ADCC).
Etanercept is a glycosylated fusion protein that contains a form of the p75 TNF receptor that binds to the inflammatory mediator, TNF. It is indicated for rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis, ankylosing spondylitis and plaque psoriasis [16].
Etanercept (Enbrel) demonstrated major differences in the glycosylation profile and in the amount of basic variants present in the molecule from 2009 to 2010 [9]. These types of changes are not unusual. Enbrel has been manufactured at multiple sites by several sponsors or contract manufacturers [17]. Glycosylation modifications are expected for every change in manufacturing location. Despite changes in these reference products, there was no change in product labelling or marketed clinical indications and no need for additional clinical trials to demonstrate efficacy in any specific indication. Darbepoetin alfa (Aranesp), rituximab (Rituxan) and etanercept (Enbrel) retained all of their approved indications.
Sometimes there are challenges in the extrapolation to all clinical indications for biosimilars. Health Canada decided to grant approval to the biosimilar anti-TNF antibody, Inflectra (infliximab) for only some of the clinical indications of the reference product, Remicade [18]. Inflectra was approved for use in rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis and plaque psoriasis, but not Crohn’s disease or ulcerative colitis. Health Canada believed that differences of the biosimilar compared to the reference product in in vitro ADCC and binding to the FcγRIIIa receptor may correlate with mechanism of action in Crohn’s disease or ulcerative colitis.
However, in 2013, EMA came to a different conclusion on the same data. Inflectra was approved as biosimilar for all eight of the clinical indications of the reference product. Their decision was included in Inflectra Assessment Report [19].
‘As part of the comparability exercise it was shown that all major physicochemical characteristics and biological activities of Inflectra were comparable to those of Remicade. The CHMP [Committee for Medicinal Products for Human Use] noted a small difference in the amount of afucosylated infliximab, translating into a lower binding affinity towards specific Fc receptors and a lower ex vivo antibody-dependent cellular cytotoxicity (ADCC) activity in the most sensitive ADCC assay. This difference was, however, not considered clinically meaningful, as it did not affect the activities of Inflectra in experimental models regarded as more relevant to the pathophysiological conditions in patients.’
The EMA decision reflects that the proposed mechanism of action, for various clinical indications is speculative at this point in time and the correlation with in vitro assays is not certain. The approval for all clinical indications should be viewed in the context of totality of data on analytical, preclinical, PK, PD and clinical information. Subsequent preliminary clinical studies have demonstrated safety and efficacy in paediatric Crohn’s disease [20], ulcerative colitis [21] and inflammatory bowel disease [22].
Failure to extrapolate to all clinical indications would cause confusion and undermine the concept of biosimilars
In addition to the scientific justification for extrapolation, it may be fundamental to the implementation and clinical use of biosimilars that they receive approval for all the same clinical indications as the reference product. Failure to do so would undermine the concept of biosimilars and principles of sound science. FDA guidance states that data for a biosimilar ‘should demonstrate that the biological product is highly similar to the reference product notwithstanding minor differences in clinically inactive components. The stepwise approach should start with extensive structural and functional characterization of both the proposed product and the reference product, which serves as the foundation of a biosimilar development program[me]’ [4]. Based on a sound characterization approach it is expected that all indications will be granted to biosimilars. The foundation of biosimilars is the demonstration of analytical similarity/comparability to the reference products. Any need for clinical data only serves to confirm the expected safety and efficacy. We might expect that sometime in the future, there will not be a need for any safety and efficacy studies for biosimilars, just PK and analytical data. Some might consider safety and efficacy studies in any clinical indication as superfluous and not a good use of medical resources.
Although sponsors are allowed to seek fewer than the full list of approved indications in a biosimilar 351k application, it is not clear under what conditions this would be an advantage for a sponsor or if this is only a hypothetical issue. If after review of the totality-of-evidence, FDA cannot be certain that a product would be effective in all clinical indications, one should question whether it is truly a biosimilar. It would infer different standards for biosimilars with all indications compared to biosimilars with fewer indications.
At this early stage of biosimilar development in the US, physicians and patients need confidence that biosimilars are safe and effective. Too often, physicians are hearing the message that biosimilars will be different from the reference product. There is some microheterogeneity for all biological products, including the reference product. However, the potential differences for biosimilars have been exaggerated with regard to the potential impact on safety, purity and potency [23]. These same concerns do not arise when changes are made to the reference product and are supported by the same test methods as used for biosimilar.
It may be understandable that some physicians and groups have expressed a desire to see clinical data for every indication. That is their realm. However, as stated by FDA, analytical and other non-clinical data is the foundation for biosimilar development and provides more meaningful information compared to clinical studies. Physicians rely on FDA to assess this data and determine the similarity and approvability of the biosimilar. Most clinical trials are unlikely to detect differences in safety, efficacy or immunogenicity between a biosimilar and a reference product. When the expected difference between two products is small, it represents a significant methodological challenge and the size of the trial needed to determine potential clinical differences between the two products would need to be very large (exceeding the size of the clinical trial for the original approval). Even comparative clinical trials between different products present difficulties [24]. Clinical studies cannot be expected to distinguish subtle clinical, safety or immunogenicity differences between two products that are specifically designed to be identical. FDA approval of biosimilars for all the clinical indications of the reference product, using the same scientific approaches used when reference products make post-approval changes, would instill confidence that biosimilars are as safe and efficacious as the reference product.
In Europe, which has approved numerous biosimilars since 2006, all biosimilars are approved for all clinical indications, and all have the same Package Insert (Summary of Product Characteristics). Similarly, in the US all generic drugs have the same Package Insert as the reference product. This is because the biosimilar or generic drug is linked to the clinical data on the safety and efficacy of the reference product. Retention of this linkage of the biosimilar to the long history of safety and efficacy of the reference product in all clinical indications is key. It would be a mistake to use a different approach in the US for biosimilars that would confound the principle of biosimilarity in the medical community. It would be irrational and potentially confusing to healthcare professionals to have some biosimilars approved for only some of the clinical indications of the reference and more confusing still to have various biosimilars each approved for potentially distinct clinical indications. It would be preferable to link each biosimilar with the safety and efficacy data of the reference product for all clinical indications.
In summary, the science justifies the approval of a biosimilar for all the clinical indications of the reference product:
- The totality-of-evidence including the demonstration of high similarity with essentially the same chemical, physical, and biological properties as the reference product in addition to PK and PD bioequivalence.
- Extrapolation has been applied to essentially all changes made to reference products after approval. Any minor differences between a biosimilar and the reference product can be analogous to the minor product differences observed in the reference product over time and with manufacturing changes. In these situations there is no change in clinical indications.
- Approval for all clinical indications retains the linkage between the history of the safety and efficacy of the reference product and the biosimilar.
- If regulatory agencies cannot be certain that a product would be effective in all clinical indications, one should question whether it is truly a biosimilar.
A42 United States Code. Regulation of Biological Products. Available from: http://www.gpo.gov/fdsys/pkg/USCODE-2013-title42/html/USCODE-2013-title42-chap6A-subchapII-partF-subpart1-sec262.htm
Competing interest: This manuscript is funded by the Generic Pharmaceutical Association (GPhA). Dr Theresa L Gerrard is a consultant to many biotech companies; confidentiality agreements restrict the publication or use of their names. Mr Gordon Johnston provides consultant services to GPhA on regulatory and policy issues. Mr David R Gaugh is the Senior Vice President for Sciences and Regulatory Affairs of GPhA.
Provenance and peer review: Not commissioned; externally peer reviewed.
Authors
Theresa L Gerrard, PhD, TLG Consulting Inc, 14521 West Salisbury Road, Midlothian, VA 23113, USA
Gordon Johnston, RPh, MS, Gordon Johnston Regulatory Consultants, Olney, MD, USA
David R Gaugh, RPh, Senior Vice President, Sciences and Regulatory Affairs, Generic Pharmaceutical Association, Washington, DC, USA
References
1. U.S. Food and Drug Administration. FDA approves first generic Copaxone to treat multiple sclerosis [homepage on the Internet]. 2015 Jul 13 [cited 2015 Jul 13]. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm443143.htm
2. U.S. Food and Drug Administration. Departmen of Health & Human Services. Citizen petition denial letter from CDER to Teva Pharmaceuticals. 16 April 2015 [homepage on the Internet]. 2015 Apr 16 [cited 2015 Jul 13]. Available from: http://www.regulations.gov/#!documentDetail;D=FDA-2015-P-1050-0012
3. European Medicines Agency. ICH Topic Q 5 E. Comparability of biotechnological/biological products. CPMP/ICH/5721/03. June 2005 [homepage on the Internet]. 2006 Mar 7 [cited 2015 Jul 13]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500002805.pdf
4. U.S. Food and Drug Administration. Demonstration of comparability of human biological products, including therapeutic biotechnology-derived products. April 1996 [homepage on the Internet]. 2015 Jul 13 [cited 2015 Jul 13]. Available from: http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm122879.htm
5. U.S. Food and Drug Administration. Avonex. Summary basis of approval [homepage on the Internet]. 1998 Nov 13 [cited 2015 Jul 13]. Available from: http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/ucm086056.pdf
6. U.S. Food and Drug Administration. Quality considerations in demonstrating biosimilarity to a reference protein product. April 2015 [homepage on the Internet]. [cited 2015 Jul 13]. Available from: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM291134.pdf
7. Rosenberg AS. Effects of protein aggregates: an immunologic perspective. AAPS J. 2006;8(3):E501-7.
8. U.S. Food and Drug Administration. Guidance for industry. Immunogenicity assessment for therapeutic protein products. August 2014 [homepage on the Internet]. 2014 Aug 12 [cited 2015 Jul 13]. Available from: http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm338856.pdf
9. Schiestl M, Stangler T, Torella C, Cepeljnik T, Toll H, Grau R. Acceptable changes in quality attributes of glycosylated biopharmaceuticals. Nat Biotechnol. 2011;29(4):310-2.
10. U.S. Food and Drug Administration. Guidance for industry: scientific considerations in demonstrating biosimilarity to a reference product. April 2015 [homepage on the Internet]. 2015 Apr 24 [cited 2015 Jul 13]. Available from: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM291128.pdf
11. Hörbrand F, Bramlage P, Fischaleck J, Hasford J, Brunkhorst R. A population-based study comparing biosimilar versus originator erythropoiesis-stimulating agent consumption in 6,117 patients with renal anaemia. Eur J Clin Pharmacol. 2013;69(4):929-36.
12. Kerkhofs L, Boschetti G, Lugini A, Stanculeanu DL, Palomo AG. Use of biosimilar epoetin to increase hemoglobin levels in patients with chemotherapy induced anemia: real-life clinical experience. Future Oncol. 2012;8(6):751-6.
13. Eisen S. Safety of biosimilars: what you really need to know. DIA presentation 2011 [homepage on the Internet]. [cited 2015 Jul 13]. Available from: http://www.diahome.org/productfiles/25233/2.2%20 sandy%20eisen.pdf
14. U.S. Food and Drug Administration. Package insert Aranesp (Darbepoetin alfa) [homepage on the Internet]. 2015 Jul 13 [cited 2015 Jul 13]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2001/darbamg091701lb.htm
15. U.S. Food and Drug Administration. Prescribing information Rituxan (Rituximab) [homepage on the Internet]. 2010 Feb 19 [cited 2015 Jul 13]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/103705s5311lbl.pdf
16. U.S. Food and Drug Administration. Prescribing information Enbrel® (enteracept) [homepage on the Internet]. 2012 Dec 11 [cited 2015 Jul 13]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/103795s5507lbl.pdf
17. Gerrard TL. The science for biogenerics: is it there already? In: Advances in large scale biopharmaceutical manufacturing and scale-up production. 2nd Ed. Washington D.C.: ASM Press; 2007:35-50.
18. Health Canada. Summary Basis of Decision (SBD) for Celltrion’s Inflectra [homepage on the Internet]. 2015 Jul 13 [cited 2015 Jul 13]. Available from: http://www.hc-sc.gc.ca/dhp-mps/prodpharma/sbd-smd/drug-med/sbd_smd_2014_inflectra_159493-eng.php#non_clinical
19. European Medicines Agency. Committee for Medicinal Products for Human Use (CHMP). Assessment report Inflectra. EMA/CHMP/589422/2013. 27 June 2013 [homepage on the Internet]. 2013 Sep 30 [cited 2015 Jul 13]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002778/WC500151490.pdf
20. Sieczkowska J, Banaszkiewicz A, Plocek A, Jarzebicka D, Gawronska A, Toporowska-Kowalska E, Kierkus J. Assessment of safety and efficacy of biosimilar infliximab in children with Crohn’s disease: a preliminary report. Poster session presentation Abstract:#P430. 10th Congress of European Crohn’s and Colitis Organisation; 18–21 February 2015; Barcelona, Spain.
21. Molnar T, Farkas K, Rutka M, Bálint A, Nagy F, Bor R, Milassin A, Szepes. Z. Efficacy of the new infliximab biomarker CT-P13 induction therapy on mucosal healing in ulcerative colitis patients. Poster session presentation Abstract:#P603. 10th Congress of European Crohn’s and Colitis Organisation; 18–21 February 2015; Barcelona, Spain.
22. Gecse K, Farkas K, Lovasz B, Banai J, Bene L, Gasztonyi B, Golovics P, et al. Biosimilar infliximab in inflammatory bowel diseases: first interim Results from a prospective nationwide observational cohort. Poster session presentation Abstract:#P314. 10th Congress of European Crohn’s and Colitis Organisation; 18–21 February 2015; Barcelona, Spain.
23. Weise M, Kurki P, Wolff-Holz E, Bielsky MC, Schneider C. Biosimilars: the science of extrapolation. Blood. 2014;124(22):3191-6.
24. Temple R. A regulator’s view of CER. Clinical Trials. 2011;10.1177/1740774511422548
|
Author for correspondence: Theresa L Gerrard, PhD, TLG Consulting Inc, 14521 West Salisbury Road, Midlothian, VA 23113, USA |
Disclosure of Conflict of Interest Statement is available upon request.
Copyright © 2015 Pro Pharma Communications International
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.



One Reply to “Biosimilars: extrapolation of clinical use to other indications”