The rate of successful development, regulatory approval and marketing of both new and follow-on biological treatments has continued to accelerate despite, and in some cases because of, a seemingly endless list of disturbing world events. This GaBI issue contains manuscripts discussing a variety of topics that are already or promise to be critical to maintaining this progress.
Interchangeability and substitution are related, but very distinct terms with respect to both biosimilars and generic drug products. The first Commentary by Rieger et al. from Western Sydney University details what the authors describe as the misleading use of the terms in promotional materials used by some competing biosimilar product manufacturers in Australia. The authors claim that the confusion created by such promotional materials as well as by the Australian Government’s ‘substitution’ rules have limited the uptake of biosimilars. They propose that the preferred solution to this problem is that physicians and pharmacists need to collaborate and then clearly communicate, ‘the boundaries, clinical goals, appropriate approaches to biosimilar substitution …’ The authors acknowledge that such an approach would require ‘substantial efforts’ and that, ‘there are no specific roadmaps’ for even opening discussions of such a collaboration. They suggest that the first step is to simply, ‘pick up the phone and strike up a conversation’. I totally agree with the need for increased and improved physician/pharmacist interactions concerning these issues. However, while I have minimal personal experience with Australian healthcare realities, I am skeptical that either physicians or pharmacists have the time or financial incentives to engage in such activities. I believe strongly in the need to base decisions on the answer to the WIIFM (What’s in it for me?) question. In my view, until/unless these busy professionals are compensated for such collaboration, those most likely to benefit from increased biosimilar uptake; health insurers and governments who are paying for the use of biologicals, must instead take responsibility for improving substitution rules, educating the public, controlling any misleading product promotion, and providing reimbursement for the time spent by providers promoting more rational medically/pharmaceutically indicated product selection.
Interchangeability is also the focus of the first Original Research by Mr Yuqi Li and Professor Dr Shein-Chung Chow from the Department of Statistics at Duke University. The authors present details of a statistical method, the interchangeability index. They claim their methods can predict, with a specified level of statistical assurance, whether a follow-on product, provided it meets certain specific criteria, would, ‘produce the same clinical result as the reference product in any given patient’. The authors make clear that the index is ‘only practical for a valid crossover switch design’ and that it only addresses the first interchangeability requirement of the Biologics Price Competition and Innovation Act of 2009 (BPCI Act). They present the results of multiple in-silico simulations that support their claims. They acknowledge the need for validation of their methods by performing Food and Drug Administration (FDA) approved switch or alternation design studies. Because of my limited statistical expertise, the decision to publish this manuscript was based solely on the opinions of external reviewers, but if/when such validation is provided, the methods might be used to decrease the number of clinical studies required to declare a biosimilar product to have met the criteria for interchangeability. I would be especially appreciative of any comments from readers, whether positive or not, about the validity or potential of the methods proposed.
The second Original Research by Piñeiro et al. presents an evaluation of the chiral switch ‘evergreening’ strategy used by the manufacturer (AstraZeneca) of omeprazole and esomeprozole. A very large number of common non-biological medications are racemic mixtures. Examples other than omeprazole include ibuprofen, cetirizine, ofloxacin, ketoprofen and fluoxetine. When the patent expires for an originator product that was originally marketed as a racemic mixture, it may be possible for the manufacturer to exclusively market a single enantiomer that is present in the racemic mixture (the switch strategy). Occasionally the single enantiomer has superior pharmaceutical characteristics and therefore produces superior clinical efficacy or less toxicity. Often however there is no rational justification for switching from a similarly effective racemic mixture to the patent protected, more expensive single enantiomer. As described in this case study, gaining marketing approval for the follow-on single enantiomer allows the manufacturer to benefit from the reputation and market share of the racemic mixture while gaining extended marketing exclusivity. Even if the removed enantiomer is merely inactive; the marketing can merely emphasize that an inactive or much less active chemical has been removed. When successful, such a marketing strategy can produce enormous profits as evidenced by the commercial success of esomeprozole. These strategies are likely to continue to produce difficult to justify healthcare costs unless/until payors develop successful ways to educate and convince both patients and prescribers to resist any unjustified use of such products. Hopefully, publishing manuscripts that explain the strategy will be part of the solution to this problem.
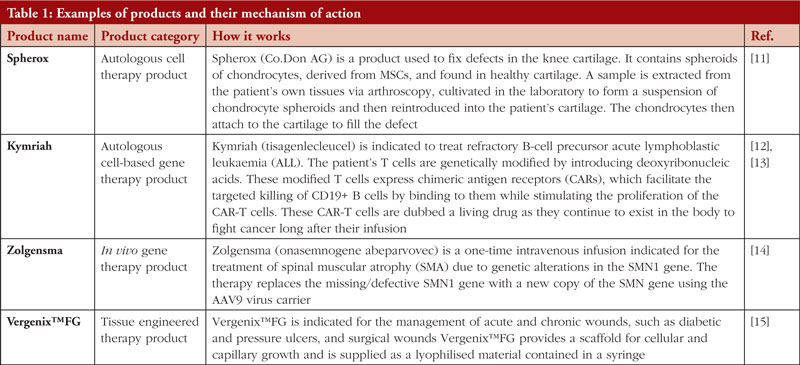
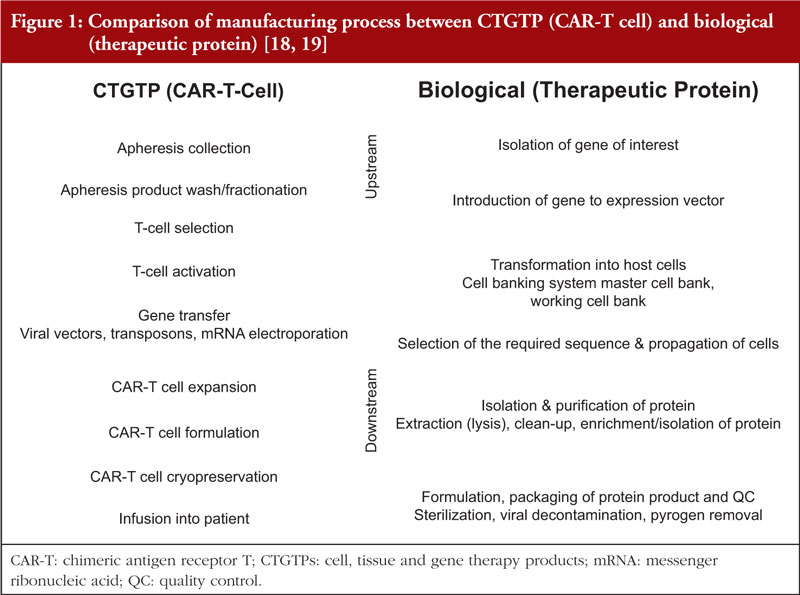
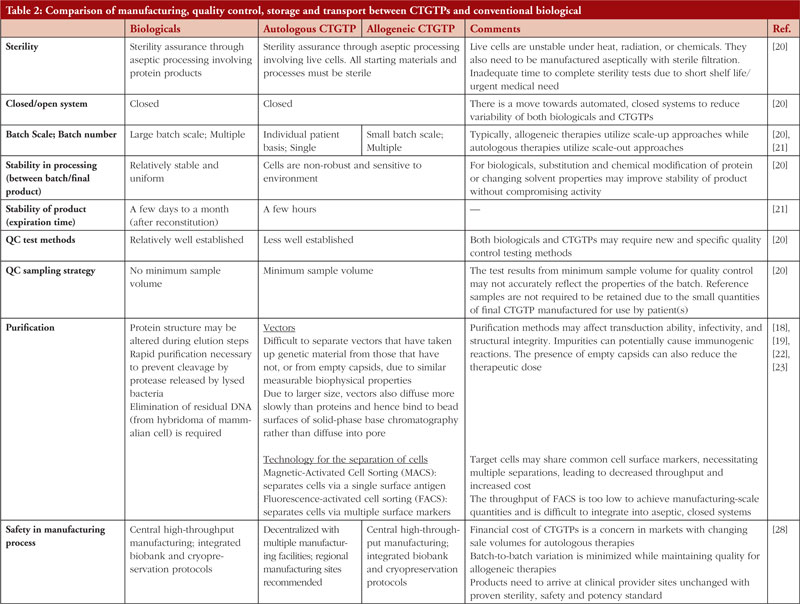
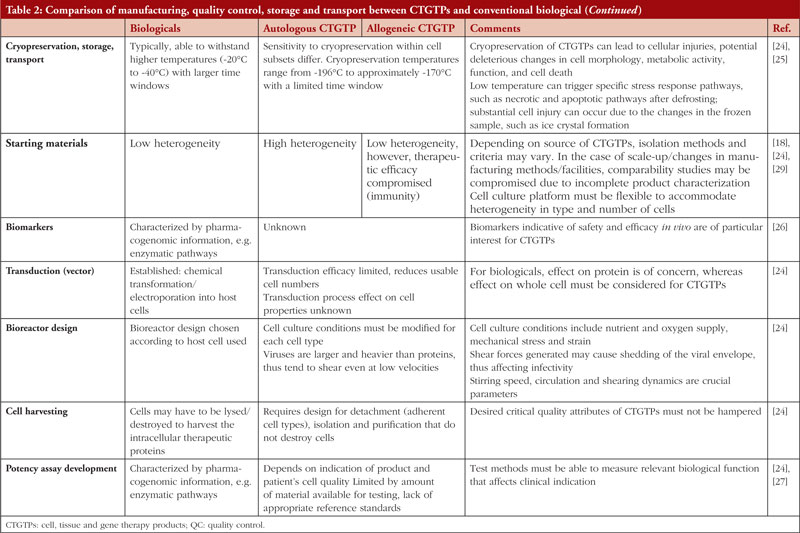
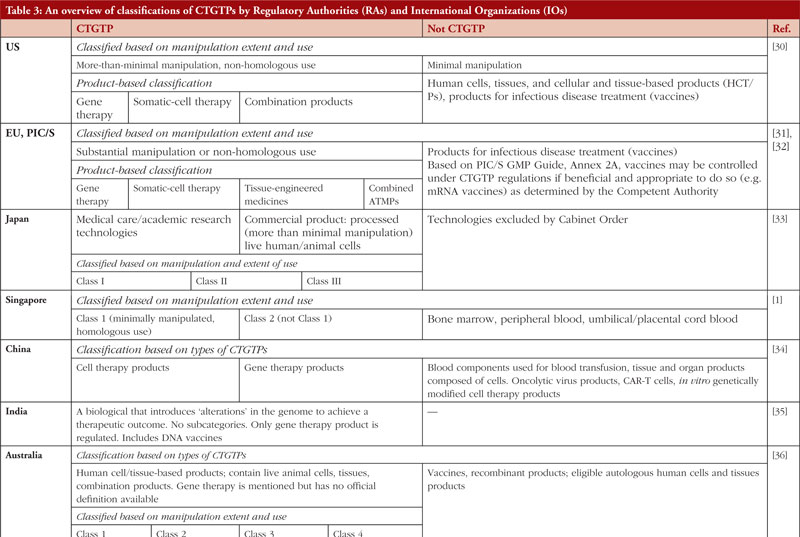
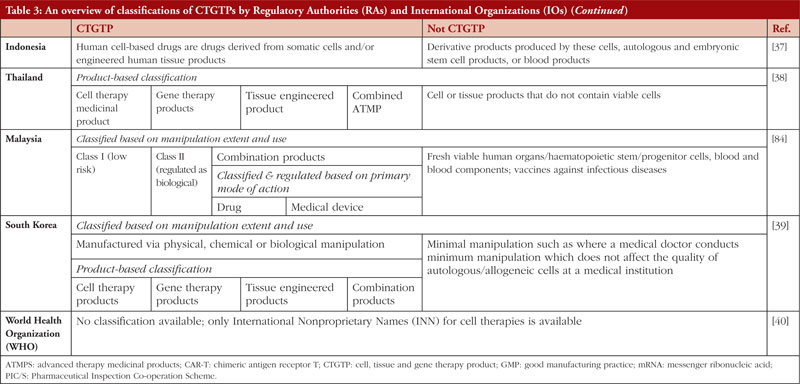
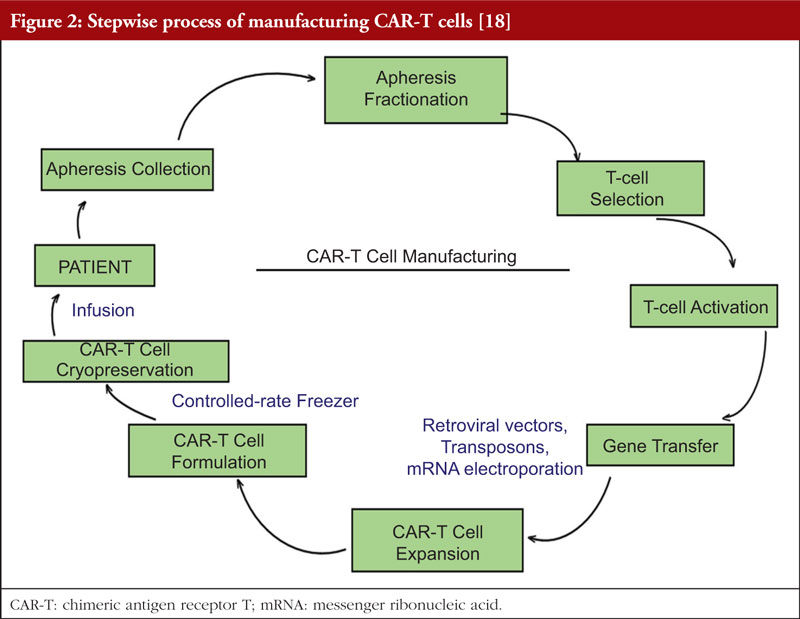
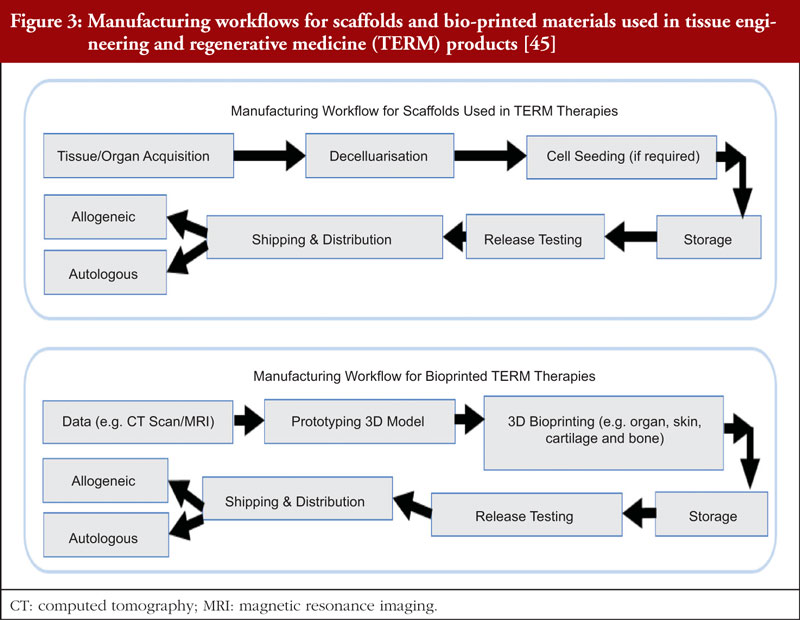
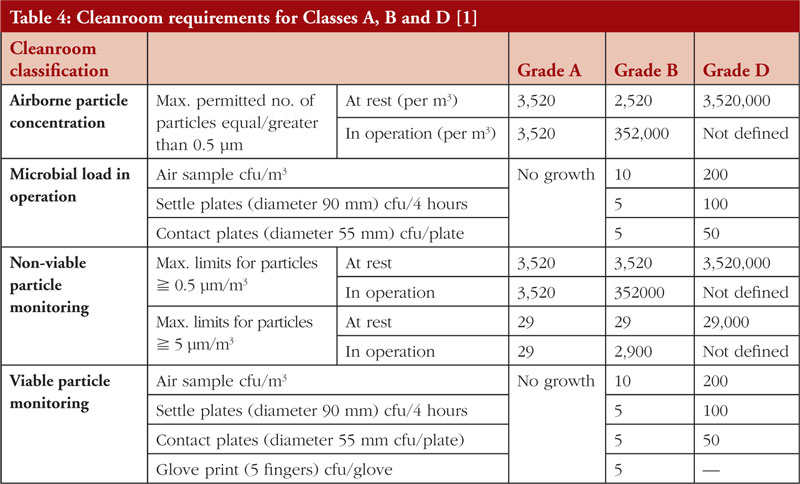
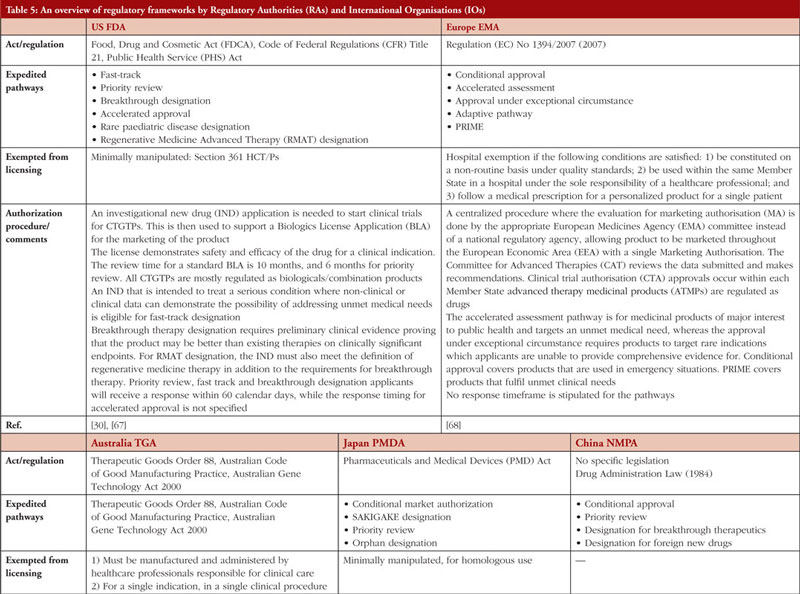
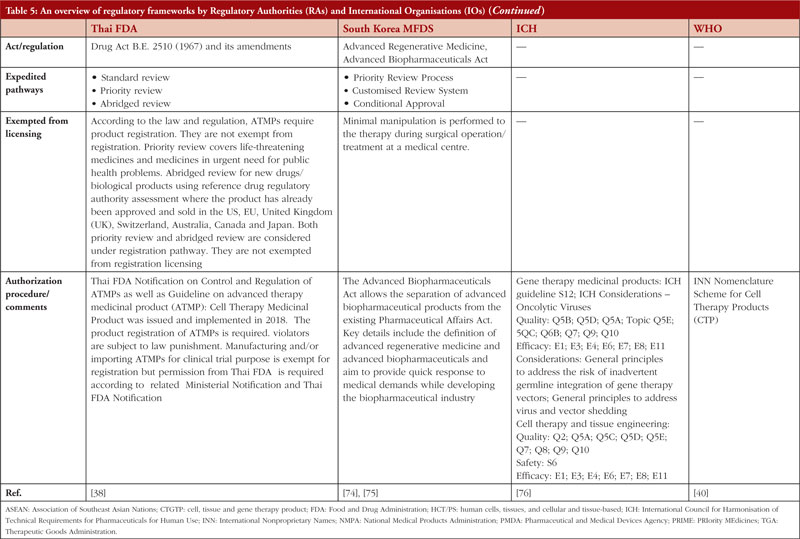
The Review Article by Adjunct Associate Professor Hoch et al. from Singapore covers, in detail, the manufacture, testing and regulation of the currently small, but rapidly growing number of important cell, tissue and gene therapy products (CTGTPs). The authors review how some CTGTP products work, the challenges associated with their manufacture, testing, quality control, and regulatory approval. Differences are reviewed that exist between CTGTPs and traditional biological products as well as the regulatory, manufacturing, quality assurance, technology, expertise and manpower issues these differences create. Finally, the authors propose potential solutions to these problems, including development of global regulatory frameworks, international regulatory harmonization, outsourcing of manufacturing expertise, and incorporation of automated manufacturing techniques. They also briefly discuss the need to provide expedited access to these important, but extremely expensive and often single patient, therapies, especially in resource poor environments. The manuscript, in my view, is required reading for anyone interested in this rapidly expanding therapeutic class; one that contains a growing number of products that provide revolutionary, often lifesaving, treatments for a growing list of both rare and common diseases.
The final, Sponsored Article summarizes an online roundtable discussion of how ‘front-loading’ of improved analytical, structural, and functional characterization of biological products can be used to reduce biosimilar development costs and decrease the number of clinical trials needed to obtain marketing approval (registration) of biological products in the UK. The speakers are all experts in this area who are actively involved in providing these services or advising the pharmaceutical industry on the development and application of such analytical techniques. While it is not clear how effectively such ‘front loading’ would decrease the number of clinical trials necessary to obtain approval outside the UK, the techniques mentioned clearly have great global potential to improve the non-clinical characterization and comparison of various biological products by both regulators and manufacturers.
Professor Philip D Walson, MD Editor-in-Chief, GaBI Journal
Disclosure of Conflict of Interest Statement is available upon request.
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Abstract:
An online roundtable discussion entitled ‘Front-loading biosimilar development with analytical characterization’ was hosted by BioPharmaSpec. The panellists discussed different regulatory approaches to the clinical trials needed for approval and how this can affect structural and functional characterization; the best way to ‘front-load’ characterization
Submitted: 18 June 2022 Revised: 19 July 2022; Accepted: 20 July 2022; Published online first: 29 July 2022
Introduction
Since the legal frameworks for biosimilar approvals were established in Europe in 2003 [1] and the US in 2009 [2], the use and uptake of biosimilars has increased across the globe. There have now been many years of biosimilars development, and the process of getting this class of drugs to market is being continually examined.
Multiple global regulatory guidelines require in-depth analysis to demonstrate that the biosimilar is similar enough to the originator in terms of structure, composition, and in-vitro activity, in addition to clinical trials to compare pharmacokinetics (PK) and examine possible clinical inequivalence. Questions are now being asked regarding the need for extensive clinical trials and whether it is more appropriate to front-load biosimilar drug investigations with risk-based analytics [3, 4].
An online roundtable discussion entitled ‘Front-loading biosimilar development with analytical characterization’ was recently organized and held by BioPharmaSpec.
BioPharmaSpec is a global contract research organization (CRO), led by industry experts in the field of mass spectrometry, specializing in the structural, physicochemical, and biophysical characterization of biopharmaceuticals such as biosimilars.
The roundtable was chaired by Dr Fiona Greer, an independent consultant with over 35 years’ experience in glycoprotein analysis and previously a founding Director of M-Scan and Global Director of Biopharma Services Development, SGS. Dr Greer was joined by three panel members, Dr Richard Easton, Technical Director for Structural Analysis at BioPharmaSpec, Dr Dan Mamelak, Founder and President of Custom Biologics, and Dr Marius Schmid Chief Executive Officer of Zentriforce Pharma. The panel discussed how detailed structural and functional investigations, as part of a comparability exercise, can be front-loaded in a biosimilar development programme to improve confidence levels in the nature of the biosimilar, reduce development costs and, in some circumstances if guidelines permit, reduce the requirement for full clinical trials. The premise of the discussion was that technological advances in hardware and software mean that detailed investigations can now take place in all aspects of primary and higher order molecular structure and the subsequent impact that any modifications can have on functional biological activity.
Roundtable key issues
During the roundtable, the following key issues were discussed:
The different regulatory approaches to the need for full clinical trials and how this can affect structural and functional characterization.
The best way to “front-load” characterization in comparability studies.
Orthogonality and its role in reducing biosimilar development costs.
How to develop an integrated strategy for structural and functional data assessments.
The panel members gave their opinions through their answers to the three questions listed below.
Certain regulatory authorities are taking a different view on the necessity of comparative clinical efficacy trials. How do you think this impacts the analytical and functional work performed as part of drug development? Dr Easton was the first to answer the question. He highlighted the fact that traditionally, for a biosimilar to be approved, it is compared to an innovator reference product. However, now that many biosimilars have been approved, there is a large body of historical data on multiple biosimilars themselves. He noted that, in a post-Brexit world, the UK’s health authority is reconsidering biosimilar evaluation and the potential to reduce reliance on clinical trial data in favour of knowledge of structural and functional properties. To do this, structural and functional information must be very robust.
Dr Schmid followed on by noting that, when it comes to removing clinical studies, the question is: who will take the risk and do this first? Although the UK is considering removing the need for clinical trials of biosimilars, the United States Food and Drug Administration (FDA) and the European Medicines Agency (EMA) are not at present, so clinical trials will still need to be done for products to be approved outside the UK.
In the UK, the biosimilar guideline provides a clear outline of the requirements and needs for clinical studies. The European Medicines Agency (EMA) follows a similar approach to the UK. Although the US regulatory stance on biosimilars may differ from that of the UK and the EMA, the US FDA can be flexible in its decisions. Nevertheless, clinical trials remain a crucial requirement for the approval of biosimilar products in both Europe and the US unless their omission can be justified by the applicant.
Dr Schmid also stated that, to expand biosimilarity study data, it could be possible to shift everything to a good manufacturing practice (GMP) environment, or to get larger statistical samples. However, he highlighted that neither seem to be completely necessary, but they might be an option to increase the trust in data. He also made the point that we have a lot of historical data on the biosimilars themselves and it might be interesting to compare new with old biosimilars as well as to reference products.
Dr Mamelak concluded the answers to this question by noting that regulatory agencies want to make it less expensive to produce biosimilars, thus reaching a wider market. With the changing approaches of some regulatory agencies, it is likely that the decision-making process will rely more on robust structure/function packages. This will help remove the need for animal and PK testing that are costly to perform and, it could be argued, unethical. Thus, moving forward, it will be important to rely on historical and empirical data.
What is the best way to develop a front-loaded characterization study? How can you build orthogonality into your approach? Dr Schmid highlighted that, when carrying out structural assessments of biosimilars, accuracy is the most difficult aspect to assess and the need for orthogonal methods is key. He noted that, ‘aggregation analytics are often needed and it is common to perform three different techniques’. In many cases, orthogonal information can be obtained, but accuracy can be harder to achieve. He concluded by noting that one way to ensure accuracy is to run positive control samples.
Dr Mamelak noted that, although orthogonal tests are key for structural testing, there isn’t always the same need for orthogonal approaches in functional analyses. He noted, ‘with functional testing, molecules are received that are known to be structurally sound and the mechanism of action is what needs to be measured’. At this point in the analysis of biosimilars, orthogonal testing is no longer needed due to the emergence of very sophisticated recombinant cell lines that are used as the target cell line for these biological molecules. In reference to these assays, he concluded by noting, ‘if the molecule works the way it’s proposed to, the cell line glows and the glow is measured’.
He also highlighted that, although it is not important to carry out orthogonal tests within functional testing, it is important to qualify the assay against a reference product to ‘show that the biosimilar is similar’. When it comes to quality, it is important to run assays under good laboratory practice (GLP), or GLP-like, conditions. In summary, Dr Mamelak noted that the emergence of sophisticated recombinant cell lines and inclusion of a reference standard means orthogonal approaches to measure mechanism of action are not critical, which streamlines the functional characterisation plan and, in turn, reduces costs.
Dr Easton noted that orthogonality is crucially important for the structural and physicochemical types of analyses carried out by BioPharmaSpec. He highlighted that such tests are needed to produce a self-supporting dataset so that all aspects of the data can be relied upon. There are various orthogonal techniques employed at BioPharmaSpec, see Table 1. He noted, ‘to design an orthogonal experiment, it is key to understand what each technique can and can’t do so that you can deduce solid conclusions, a concrete package and in-depth knowledge of the molecule’.
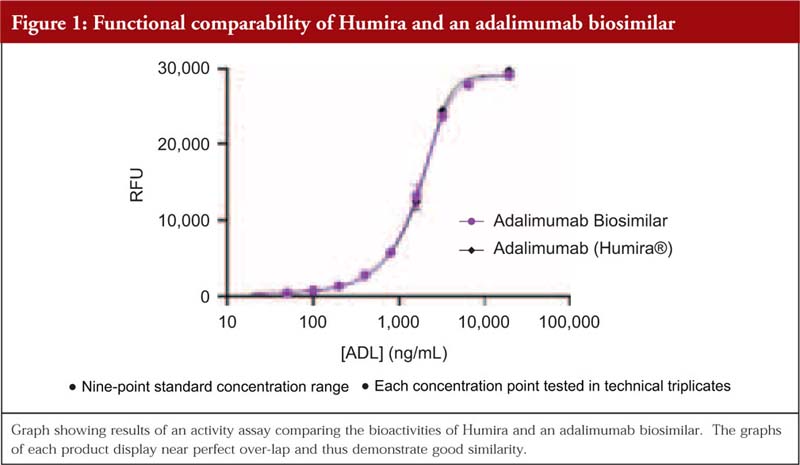
Dr Mamelak then added that, when it comes to functional testing, it is advantageous if the product’s structure has already been well-defined. When the comparability study is carried out within a cell-based assay, a curve is often produced to demonstrate how similar a biosimilar is to the reference. He shared the example of a comparability study of adalimumab biosimilar/originator behaving similarly, here the graphs overlap and thus demonstrate that they are behaving similarly. In addition, he remarked that the graph also showed that the structural analysis carried out to determine potential differences prior to the functional testing had been done very well.
Lastly, Dr Mamelak noted that in some cases, the buffer of the biosimilar can be different to that of the reference product and this can cause differences. Here, a cell-based functional assay is a useful tool to determine if there are any effects on functional properties, see Figure 1.
What is your experience of linking analytical characterization to function, i.e. an integrated strategy? What about the challenges of performing these correlations between the originator and biosimilars? Can you illustrate with examples? Dr Mamelak highlighted that this question touches on the ‘holy grail’ of developing a biosimilar package. The structure and function analyses are the driving force that will bring the cost of developing biosimilars down. A good structure-function package with orthogonal approaches at the structural phases and well-designed functional characterization of the molecule is what the regulatory agencies want to see.
From a functional perspective, the main challenge is that the assay has to show that it can pick up subtle differences and must be able to confirm differences and similarities. An assay must be sensitive enough to show that differences can be captured, and any differences must be explained. He noted that it is important to ask: ‘Can the assay pick up differences in functional activity that are likely due to differences in structural properties?’ He then demonstrated this by giving some examples of cell-based bioassays. Overall, he stressed that a solid structure-function package is the key driving force to help bring the cost of biosimilar development down.
Dr Schmid provided a case study from aggregation analyses where a generic drug (cyclosporine) performed differently to the originator and they found, by examining oil drop distribution, that the issue was in the micellar structure of the Tween.
Dr Easton concluded the answer to the final question by noting that, to get a good understanding of the structure-function relationship, you have to know your assays and your product well enough to be able to understand any differences you might see and put them into the context of your development programme. Developing good lines of communication between the scientists carrying out the structure and the functional analyses is crucial to front-loading analytics and truly defining biosimilarity.
Conclusion
Dr Greer concluded that it is clear that detailed structure-function investigations as part of the comparability exercise can give great confidence in the nature of the biosimilar, providing information from which risk-based assessments can be made. Results from orthogonal methods can provide a meaningful insight into how similar the biosimilar is to the originator and potentially reduce the requirement for full confirmatory clinical trials. Overall, structural-functional data should be viewed in tandem for full understanding in integrated studies to enable a reliable assessment of biosimilarity.
Funding sources
This paper is funded by BioPharmaSpec Ltd (www.biopharmaspec.com).
Editor’s comments
The roundtable discussed how biosimilar manufacturers might be able to decrease the number of clinical trials required for registration now that the UK is no longer part of the EU. It was noted that until/unless the FDA and/or EMA change their current approach the need for clinical PK, safety and efficacy studies is unlikely to be decreased by what has been proposed in the UK.
References 1. GaBI Online – Generics and Biosimilars Initiative. Biosimilars approved in Europe [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2022 Jul 19]. Available from: www.gabionline.net/biosimilars/general/biosimilars-approved-in-europe 2. GaBI Online – Generics and Biosimilars Initiative. FDA approves its first biosimilar [www.gabionline.net]. Mol, Belgium: Pro Pharma Communications International; [cited 2022 Jul 19]. Available from: http://www.gabionline.net/biosimilars/news/FDA-approves-its-first-biosimilar 3. Bielsky M, Cook A, Wallington A, Exley A, Kauser S, Hay JL, et al. Streamlined approval of biosimilars: moving on from the confirmatory efficacy trial. Drug Discov Today. 2020;S1359-6446(20)30343-3. doi: 10.1016/j.drudis.2020.09.006 4. BioPharmaSpec. Biosimilars roundtable discussion with analytical characterization experts [homepage on the Internet]. [cited 2022 Jul 15]. Available from: https://biopharmaspec.com/biosimilars-roundtable-analytical-characterization/
Author: Richard L Easton, BSC (Hons), DIC, PhD, Technical Director, BioPharmaSpec Ltd, Suite 3.1 Lido Medical Centre, St Saviours Road, St Saviour, Jersey JE2 7LA
Disclosure of Conflict of Interest Statement is available upon request.
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Author byline as per print journal: Yuqi Li, BS Pharm; Shein-Chung Chow, PhD
Abstract:
A biosimilar product is a biological product which is highly similar to an existing reference product in structure and function and has no clinically meaningful difference in terms of safety, purity or potency. Under the Biologics Price Competition and Innovation Act of 2009 (BPCI Act), the Food and Drug Administration (FDA)-approved interchangeable biosimilar products can be expected to produce the same clinical result as the reference product in any given patient. In practice, although it is impossible to demonstrate that a proposed interchangeable biosimilar can meet this criterion due to differences in physiological conditions of patients and subtle differences between products, it is possible to demonstrate that the interchangeable biosimilar can produce the same clinical result as the reference product in any given patient with certain assurance. In this article, we derived a statistical method, which we refer to as an interchangeability index, for evaluating of the interchangeability of a biosimilar product with a certain statistical assurance. The proposed method was evaluated via extensive simulation studies. The results indicate that when the ratio of mean clinical results produced by test and reference product is within a narrow limit and the clinical results have only moderate variability, higher interchangeability index would suggest the test products are likely to meet the criteria for biosimilar interchangeability.
Submitted: 30 June 2022; Revised: 28 July 2022; Accepted: 29 July 2022; Published online first: 11 August 2022
Introduction
Biological products are typically large, complex, biologically active molecules produced by living systems, such as micro-organisms, plants or animal cells. These bioproducts are diverse and they may have preventive, diagnostic and therapeutic functions for diseases. Unlike chemical drugs made by non-biological, synthetic processes, biological products which are complex biomolecules, the manufacture of which produces some expected slight differences. Biological products are regulated by the US Food and Drug Administration (FDA), and the review and evaluation of manufacturing performed by FDA can help ensure that the produced biological products have consistent clinical performance [1]. Reference products are biological products approved by FDA based on extensive pre-clinical and clinical safety and efficacy data. A biosimilar product is defined as a biological product that is highly similar to an existing reference product in structure and function and has no clinical difference in terms of safety, purity or potency [1].
As an increasing number of biosimilars become available on the market, more drug use options are provided by introducing competition, the cost of treatment has been reduced. Thus, the medical treatments have become more accessible to patients. Given the availability of numerous options for drug use, it is natural to consider the issue of interchangeability between biosimilars. As indicated in the additional requirements by the Biologics Price Competition and Innovation Act of 2009 (BPCI Act) [2], a proposed biosimilar product which is considered to be an interchangeable biosimilar product for a reference product must satisfy two criteria. First, the biosimilar product can be expected to ‘produce the same clinical result as the reference product in any given patient’. Second, the risk regarding safety and reduced efficacy of switching or alternating between the reference and the interchangeable biosimilar product is not greater than the risk of using the reference product without switching or alternating. The demonstration of a proposed interchangeable biosimilar product is highly similar to a reference product in producing clinical results. In other words, the proposed biosimilar can meet the criteria, and a valid clinical trial design such as a crossover design must be conducted [3].
Considering the first criterion, in practice, it is impossible to demonstrate that a proposed interchangeable biosimilar product can produce the same clinical result as the reference product in any given patient. This could be due to various reasons, such as the fact that the underlying pathology and physiological conditions are not identical in each patient, and the fact that there are slight, acceptable within-product differences in the manufacturing process of the biological product from batch to batch. However, it is statistically possible to demonstrate that the interchangeable biosimilar can produce the same clinical result as the reference product in any given patient with certain assurance. Towards this goal, we mainly focused on the first criterion, and we proposed a statistical approach by evaluating the probability that reference and test products produce the same clinical results in any given patient. When this probability exceeds a prespecified threshold, we then claim that the biosimilar product is interchangeable.
In section 2, some rules regarding clinical data and basic study designs for switching/alternation in interchangeable biosimilar products are introduced. In section 3, statistical methods for estimating the proposed probability, which is referred to as an interchangeability index, are derived theoretically. In section 4, extensive simulation studies are performed to evaluate the proposed method. In section 5, conclusions are provided based on the methods and simulation study results.
Criteria and study design
Log-transformed data and therapeutic index limit Given the clinical results are considered in related studies, pharmacokinetic data are typically collected usually to assess the interchangeability using statistical methods with some prespecified criteria. The raw pharmacokinetic data may often not be symmetrically or normally distributed, and a large range of the data may be noted. To address these issues and to make it easier to process the data for biostatistics analysis, FDA 1992 and 2001 guidance [4, 5] suggest considering the logarithmic transformation of pharmacokinetic data. Log-transformed data do not change the nature of the data or the correlations between variables. Rather, this transformation compressed the range of the data, making it easier to perform statistical analysis, and the effect of outliers is also reduced [5]. In practice, log-transformed pharmacokinetic data tend to have normal or approximately normal distributions, representing another important reason for the use of logarithmic transformation of data. The standard deviation of log-transformed data is often 1% of the standard deviation of the raw data. In addition, the logarithmic transformation could almost eliminate the problem of heteroskedasticity in the analysis.
Recall that our goal is to evaluate the probability that a biosimilar product produces the same clinical results in any given patient as a reference product. Although it is unlikely that the two products will produce identical clinical outcomes, the clinical results from the two products are probably within a narrow limit. Considering the ratio of the clinical outcomes, which are numeric data, if the clinical results are almost identical, the ratio should be close to 1. A limit of the therapeutic index can be set for the ratio. That is, if the ratio is within a narrow limit including 1, we may consider the two products as interchangeable. Since the log-transformed data are used in the analysis, the limit of the therapeutic index between the reference and biosimilar product should satisfy L1 × L2 = 1, thus there will be symmetric limits within the log-transformed space. Of course, given that biological products target a large population, in addition to the mean of clinical results, the variability due to subject-by-product should also be considered. We will discuss this information in later sections.
Switching design As noted in the introduction, to determine whether a proposed biological product is an interchangeable biosimilar product, a valid clinical study design is necessary. FDA defines the switching as a single switch, whereas alternation is defined as multiple switches between two biological products, respectively [3]. An adequate design can be useful to evaluate whether a proposed biosimilar product can produce the same clinical result in any given patient as a reference product and evaluate the risk in terms of efficacy and safety with or without switching/alternation.
The FDA guidance about biosimilar interchangeability recommends a 2 × (m + 1) crossover design [3], where m is the number of switches. For a single switch, an adequate crossover design consists of two sequences which are RT and RR, where R represents the reference product and T represents the test product. This design is denoted by (RT, RR), which can evaluate the effect and safety of the switch from R to T and no switch. The relative risk of product use between the switch and no switch can also be assessed. When more than one switch occurs (m ≥ 2), a 2 × (m + 1) crossover design is still necessary. For example, when it switches twice (m = 2), a 2 × 3 crossover design consists of the two sequences which are RTR and RRR. This design is denoted by (RTR, RRR). This design is able to evaluate the efficacy of the switch from R to T and then to R and the efficacy of no switch. The relative risk can also be estimated under the study design.
In this case, in addition to the 2 × (m + 1) crossover design, a n-of-1 trial design has become an alternative popular design in recent years [6]. In a n-of-1 trial, a single subject is the entire trial. Random allocation is used to determine the order of the treatments given to a subject. This trial can be used to evaluate the difference in treatment effect within the same individual when multiple treatments are assigned at different periods. [7, 8] In fact, the n-of-1 trial has a nature of crossover design which can assess the relative risk between switching/alternation and without switching/alternation.
Statistical method
Interchangeability index Without loss of generality, we assume that the data from clinical trials have been logarithmically transformed and follow a normal distribution with specified mean and variance. Let YR and YT be the clinical results of the reference product and the test product, where R = log YR and T = log YT follow normal distributions with means µR, µT and variances σ2R, σ2T, respectively. Referring to the idea of using P(X < Y) [9, 10] to assess the interchangeability between two biological products, we propose the following probability as an index to evaluate the consistency of the clinical results of the reference and test products:
Where 0 < L1 < 1 and L2 > 1, L1 and L2 are defined as the acceptable lower bound and upper bound of the therapeutic index, respectively. Based on the characteristics of logarithm transformation, the limit of therapeutic index between the reference and biosimilar product should satisfy L1 × L2 = 1, then the transformed limits will have the same distance to 0 (after log-transformation, log 1 = 0 ). The proposed interchangeability index refers to the probability p. Denoting F as the ratio of YT and YR , as F converges to 1, p tends to 1. The probability p converging to 1 indicates that the two products can be considered as identical in terms of producing clinical results. The ratio F converging to 1 will require a high degree of clinical consistency between the two products for any given patient, which is usually diffi cult to realize in practice.
Estimate of interchangeability index Under the normal distribution assumption of R = log YR and T = logYT, where R ~ N (µR, σ2R) and T ~ N (µT, σ2T), the probability p can be derived as the form below:
where Φ(z0) = P (Z < z0), Z is a standardized normal random variable. Thus, the interchangeability index p is a function of the parameters ~θ = (µT, µR, σ2T, σ2R). Assuming that in a study design, the observations are presented by Ri = log YRi, i = 1, …, nR and Ti = log YTi, i= 1, …, nT. Then the maximum likelihood estimator (MLE) of the probability p can be derived as following:
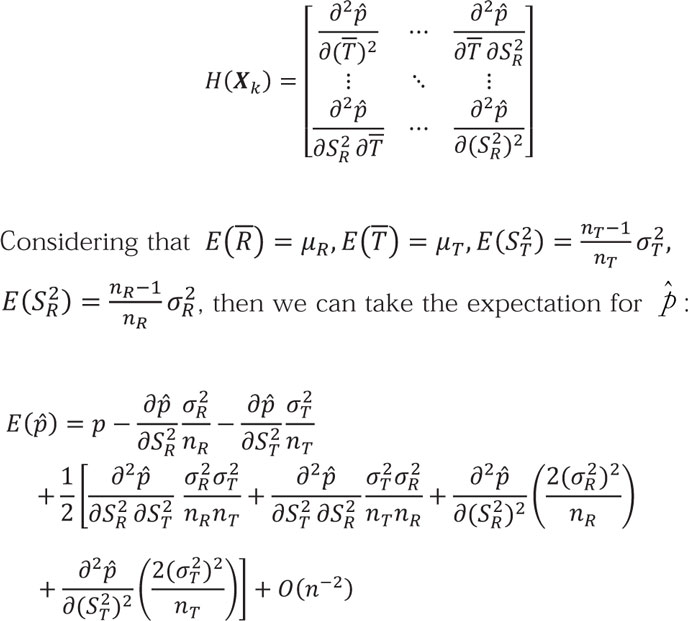
Based on the normality and large sample assumptions, there are still some asymptotic statistical results holding. Since the derived formula for the estimate of p is very complex, we consider using the Taylor expansion formula to approximate p locally. Recall that:
Applying Taylor expansion of at p, in other words, at X = Xk = (μT, μR, σ2T , σ2R), we can get:
Where H (Xk) is Hessian Matrix.
We can further derive the first term of this Taylor expansion as the leading term. In addition, to simplify this case, we will only focus on the leading term in expectation, so that the expectation for can be rewritten as the following formula:
Following the same idea, we can also get the variance of :
To simplify these formulas, let E() = p + B(p) + O(n–2), where B(p) is the leading term in the expectation formular mentioned above and is also the bias between and p. Since O(n–2) is the reminder term, in statistics we can omit its effect. Similarly, let Var () = C(p) + O(n–2), where C(p) is the leading term of Var ().
Since we assume the large sample in study, using Slutsky’s Theorem,
In this situation, applying the expectation and variance derived above, we can furthermore derive that:
where B() and C() are the estimates of B(P) and C(P). As the sample size increases to infinity, B(P) converges to 0 and then will be asymptotically unbiased.
Based on these theorems above, an approximate (1 – α) 100% confidence interval (CI) for the interchangeability index P) and C(P can be obtained. Since the proposed probability indicates to what extent the test and reference products are identical, in other words, interchangeable, in terms of producing clinical results in comparable population, we only focus on the lower bound of the confidence interval. Thus, we can construct a one-side (1 – α) 100% CI for interchangeability index P as following:
Based on the data from a switching design, we can calculate , the point estimate, and L(), the lower bound of a one-sided (1 – α) 100% CI for the interchangeability index p. Given significance level α and a pre-specified threshold β, we can compare β and L(). If L() ≥ β, we could conclude that the test and reference biological products are interchangeable.
Simulation study
For a valid statistical analysis of biosimilar interchangeability, it is necessary to perform the statistical procedure under some prespecified acceptance criteria. We will construct a 95% CI for the proposed interchangeability index described previously. If the 95% CI lower bound is greater than a prespecified threshold β for interchangeability, we will claim that the test product is interchangeable for the reference product.
In this section, we will perform simulation studies to evaluate the performance of the proposed statistical method regarding interchangeability. We will specify different distribution parameters for the normal distribution to generate simulated experimental log-transformed pharmacokinetic data, perform statistical analysis on these data to calculate the interchangeability index and its one-sided 95% CI, and further explore the influence of the distribution parameters on the statistical results and threshold selection based on these simulations, and select the sample size for different data and thresholds.
First, we need to clarify some denotations and assumptions in this study:
(1) To provide a more specifi c context for the simulation study, we try to set concrete therapeutic index limits (L1 and L2). Considering L1 × L2 = 1, to make our simulation study more general without fi rst setting a harsh criterion, in this case, we will propose L1 = 0.8 and L2 = 1.25. (2) Let F = YT/YR, where YT and YR are the means of the clinical results produced by test and reference products, respectively. When F ∈ (0.8, 1.25) is in fact, it is possible that the two products could be claimed to be interchangeable. (3) We will assume nT = nR= n in the switch design given that crossover trial designs typically enrol a similar number of comparable subjects for both sequences. (4) We will assume σT = σR = σ given that the logarithmic transformation substantially reduces the variance of the data, so the variance of the transformed data should be approximately the same for pharmacokinetic data from comparable populations.
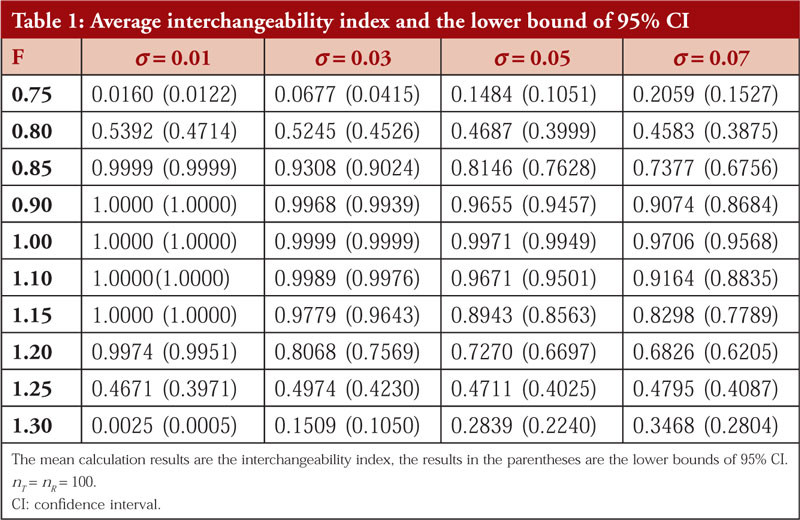
Average probability and the lower bound of 95% CI Given the different ratios of YT and YR (ranging from 0.75 to 1.30) and different standard deviations of the log-transformed data which are normally distributed (ranging from 0.01 to 0.07). We chose the sample size nT = nR = 100. As mentioned in section 2.1, logarithmic transformation can reduce the standard deviation to approximately 1% of that of the raw data, thus we select this range of σ. In addition, regardless of the scale of the raw data, as long as the ratio of YT and YR is the same, this ratio will become the same difference after logarithmic transformation. Thus, the scale of the data has no effect on the results of the simulation study. The data were generated based on the prespecified parameters F and σ for 5,000 times, and the the average probability p (interchangeability index) and the lower bound of the 95% CI were calculated.
The results of simulation 1 are presented in Table 1.
From the simulation results, we found that the interchangeability index decreases rapidly with increasing variance, meaning that a larger variance decreases the probability of two products being evaluated as interchangeable, even if the ratio of their means of clinical results is in the range of 0.8 to 1.25. It is reasonable because if a biological product produces a relatively large variance in clinical outcomes, it is an indication that it is not therapeutically stable and therefore will not be easily considered interchangeable.
Considering that σ = 0.07 expands one hundredfold to 7 as the standard deviation of the raw pharmacokinetic data, i.e., the coefficient of variation (CV) = 7%. This number represents a large variance and the lower bound of the CI is less than 90% for both cases with ratios of 0.9 and 1.1. Thus, we will not consider such a large standard deviation in subsequent simulation studies. For σ = 0.01, this standard deviation is so small that it means that the fluctuations in the data are minimal as long as the mean ratio of the clinical results produced by two products is within the range of 0.8 to 1.25 (not too close to the boundary). In addition, the interchangeability index is very high, and the test product is claimed to be interchangeable for the reference product. Thus, we will also not consider such a small standard deviation in further simulation studies.
Regardless of the chosen standard deviation, as long as the ratio F is outside the range of 0.8 to 1.25, the calculated interchangeability index is extremely small, indicating that such test products cannot generally be considered interchangeable under this statistical method. Thus, so we do not need to study the ratios outside the range of 0.8 to 1.25. In other words, this statistical method can well ensure that non-interchangeable products will not be claimed to be interchangeable. For the data in which the ratio is within the range from 0.9 to 1.1, as long as the standard deviation is not too large (e.g. σ = 0.07), the test products can be evaluated as interchangeable products for reference products under this statistical method. Thus, we do not need to continue to investigate the statistical results in this ratio range.
For further studies, we only need to focus on cases where the ratio F is between 0.8 and 0.9, 1.0 and 1.25, and only assume that the standard deviation of the log-transformed data is in the range of 0.3 to 0.5. Data with such characteristics are more meaningful for assessing the performance of this statistical method.
Changing the sample size Based on the results of simulation 1, in this simulation we focused on statistics corresponding to variance and ratios in a specific range and evaluated the performance of our statistical method. Additionally, considering that the sample size affects the accuracy of the statistical results, this study sets different sample sizes for the calculation of the interchangeability index. Given that we expect the lower bound of the 95% CI of the interchangeability index to determine whether two products are interchangeable, we will only report the lower bound of the one-sided 95% CI in this study. Similarly, for each simulation, the process is performed 5,000 times. The chosen parameters and the results are presented in Table 2.
Overall, given the variance and ratio, the interchangeability index almost still increases as the sample size increases within a certain range. When the sample size exceeds 100, the increase in the interchangeability index becomes unobvious. When the sample increases further, the value of the index almost just fluctuates without a significant increase. Therefore, considering that the switch design for biosimilar product interchangeability is usually a crossover design, a sample size of approximately 100 subjects for each sequence is appropriate based on the simulation results. Similar to the findings of simulation 1, the interchangeability index is lower when the ratio is close to 0.8 or 1.25. In general, this value cannot be increased significantly by increasing the sample size. According to the results of this simulation study, when the standard deviation is small (0.03), the interchangeability index has a relatively high probability of being greater than 80% if the ratio is in the range of 0.85–1.20. When the standard deviation is slightly larger (0.05), the interchangeability index can only reach a level of approximately 70% if the ratio is approximately 0.85 and 1.20. It is understandable that when the variance increases, the more the clinical outcomes produced by the biological product in patients fluctuate, the less likely it is to be assessed as interchangeable with the reference product.
Conclusion and discussion
For the assessment of drug interchangeability of biosimilar products, in practice, it is impossible to demonstrate that the test product can produce the same clinical therapeutic effect as that of the reference product given the difference in patients’ conditions and manufacturing differences and so on. In this article, we provided a statistical assurance that “test product has the same therapeutic effect as that of the reference product with certain assurance”. In other words, this statistical analysis assures a high probability that test product has the same therapeutic effect in any given patient, thus supporting the claim of interchangeability between test and reference products. For this purpose, following a similar idea of Chow et al. [10], a statistical method is proposed to estimate the probability of the two products producing the same clinical results (with an acceptable difference in a narrow limit).
In the simulation studies, we used 0.8 and 1.25 as the therapeutic index limits in reference to the 80/125 rule in bioequivalence for generic drugs. Indeed, the interchangeability of biosimilar products is not the same as bioequivalence of generic drugs, but similarities are noted to some extent. In practice, based on the definition of interchangeable biosimilar products, the limits might be narrower than 0.8 and 1.25. The simulation results indicate that for a ratio of two product means between 0.85 and 1.20, when the variance is not too large, the value of the interchangeability index can basically achieve 80% or greater with suitable sample size. That is, if we set an appropriate value to the threshold, the interchangeability index can be used to assess whether two biological products are interchangeable based on the data of the exchange design. However, it is difficult to claim that two products are interchangeable by calculating the interchangeability index when the clinical effects of the products fluctuate widely (large variance due to subjects by product) or when the ratio of the mean values of the two products is close to 0.8 or 1.25. For such a test product, the statistical method proposed in this study cannot yet be used as a valid evaluation tool, but this is an indicating the conservative nature of this statistical standard.
Further scenarios regarding this statistical method should be considered. Regardless of how we increase the sample size to the extent feasible in clinical trials, the value of the interchangeability index is well below 80% when the ratio is near 0.8 or 1.25. This finding is understandable. Consider a product tested has a mean clinical effect of 80% of the mean of the reference product, but the data fluctuate between patients. Here, the clinical effect produced in a large proportion of subjects will be less than 80% of the reference product. Thus, it is difficult for such a product to be recognized as interchangeable. The same is true when the ratio is approximately 1.25. For such a product, how exactly do we determine whether it is interchangeable with the reference product? This also requires further establishment of evaluation criteria based on its characteristics. In summary, the threshold for the interchangeability index and the therapeutic index limit are the main considerations when using this statistical method to claim whether a proposed biosimilar product is interchangeable for a reference product.
This interchangeability index is valid for the evaluation of biological products that meet certain conditions. However, the index in this study is only practical for switch design (a valid crossover design), and this article only addresses the first requirement for interchangeable biosimilar products according to the BPCI Act. The proposed method can be applied to switching design as recommended by FDA. To demonstrate biosimilar interchangeability, we also need to explore the relative risk between the test and reference products by performing study with a switch or alternation design. This requires further research under FDA’s recommended switching designs, either (RTR, RRR) for a single switch or (RTRT, RRRR) for multiple switching (alternation).
Competing interests:None.
Provenance and peer review: Not commissioned; externally peer reviewed.
Authors
Yuqi Li, BS Pharm, Master of Biostatistics candidate, BS Pharm Department of Biostatistics and Bioinformatics, Duke University School of Medicine, Suite 1102, Hock Plaza, 2424 Erwin Road, Durham, NC 27705, USA
Professor Shein-Chung Chow, PhD Department of Biostatistics and Bioinformatics, Duke University School of Medicine, Suite 1102, Hock Plaza, 2424 Erwin Road, Durham, NC 27705, USA
References 1. U.S. Food and Drug Administration. Guidance on scientific considerations in demonstrating biosimilarity to a reference product. April 2015 [homepage on the Internet]. [cited 2022 Jul 28]. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/scientific-
considerations-demonstrating-biosimilarity-reference-product 2. U.S. Food and Drug Administration. Biologic Price, Competition, and Innovation Act of 2009. 2009 [homepage on the Internet]. [cited 2022 Jul 28]. Available from: https://www.fda.gov/media/78946/download 3. U.S. Food and Drug Administration. Guidance for industry—considerations in demonstrating interchangeability with a reference product. 2019 [homepage on the Internet]. [cited 2022 Jul 28]. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/considerations-demonstrating-interchangeability-reference-product-guidance-industry 4. National Technical Reports Library. Guidance for Industry. Statistical approaches to establishing bioequivalence [homepage on the Internet]. [cited 2022 Jul 28]. Available from: https://ntrl.ntis.gov/NTRL/dashboard/searchResults/titleDetail/PB2010104191.xhtml 5. U.S. Food and Drug Administration. Guidance on statistical approaches to establishing bioequivalence. 2001 [homepage on the Internet]. [cited 2022 Jul 28]. Available from: https://www.fda.gov/regulatory-information/
search-fda-guidance-documents/statistical-approaches-establishing-bioequivalence 6. Chow SC, Song F, Cui C. On hybrid parallel–crossover designs for assessing drug interchangeability of biosimilar products. J Biopharm Stat.2017;27(2):
265-71. 7. Lillie EO, Patay B, Diamant J, Issell B, Topol EJ, Schork NJ. The n-of-1 clinical trial: the ultimate strategy for individualizing medicine? Per Med. 2011;8(2):161-73. 8. Davidson KW, Cheung YK, McGinn T, Wang YC. Expanding the role of n-of-1 trials in the precision medicine era: action priorities and practical consideration. National Academy of Medicine. 2018. https://doi.org/10.31478/201812d 9. Jacobs R, Bekker AA, van der Voet H, Ter Braak CJF. Parametric estimation of P(X > Y) for normal distributions in the context of probabilistic environmental risk assessment. PeerJ. 2015;3:e1164. 10. Tse SK, Chang JY, Su WL, Chow SC, Hsiung C, Lu Q. Statistical quality control process for traditional Chinese medicine. J Biopharm Stat. 2006;16(6):861-74.
Author for correspondence: Yuqi Li, BS Pharm, Department of Biostatistics and Bioinformatics, Duke University School of Medicine, 2424 Erwin Road, Durham, NC 27705, USA
Disclosure of Conflict of Interest Statement is available upon request.
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Author byline as per print journal:Chad Rieger1, MBA; Lisa Hall1, PhD; David Lim2,3, DPH
Abstract:
Bandiera et al. (2002) identified the potential for competitors’ promotional materials to use certain terms with technical meanings, such as ‘interchangeable’ and ‘substitution’, in a misleading way in Australia.
Submitted: 30 June 2022; Revised: 4 July 2022; Accepted: 5 July 2022; Published online first: 18 July 2022
The blurring of language used within the Australian Pharmaceutical Benefits Scheme (PBS) and the conflicting elements within the system contribute to the resultant tenuous uptake of biosimilar medicines in Australia.
Whilst ‘substitution’ and ‘interchangeability’ are likely to represent the same thing in the clinicians’ and consumers’ minds when it comes to small molecule generics, there is a real likelihood of confusion and subsequent delay in biosimilars uptake in Australia where such terms are used [1, 2]. The potential for confusion between ‘substitution’ and ‘interchangeability’ has real implications for the uptake of biosimilars in Australia and other countries where there is a lack of legislative definition and/or clarity of what ‘interchangeability’ entails.
There are only two mentions of ‘interchangeable’ in the enabling legislation in Australia, one with regard to the functions of the Pharmaceutical Benefits Advisory Committee (section 101, National Health Act 1953), and the second permitting the Minister to receive advice from the Pharmaceutical Benefits Advisory Committee whether a pharmaceutical may be interchangeable (section 84AG). Unlike the US, the term ‘interchange(ability)’ is not formally defined in the Australian pharmaceutical legislation [2]. Consequently, in some jurisdictions within Australia, state and territory governments have unintentionally used the terms ‘substitution’ and ‘interchangeability’ in their lay language [2]. This is likely contributing to confusion around how these terms apply to biosimilars and the implications for applications in patient care settings.
Examples of this confusion are playing out frequently and are magnified by structural elements that exist around allowable substitution within the PBS. Similar to the US Food and Drug Administration concept of the ‘Purple Book’, the Australian PBS provides a schedule of bioequivalence brands of Australian Government subsidised biological pharmaceuticals. These so-called ‘a-flagged’ biosimilars may be substituted for another brand at the point of dispensing by the community or hospital pharmacists without the requirement to reference the clinician, provided there is no explicit ‘substitution not permitted’ designation on the prescription [3]. Furthermore, pharmacists are granted the authority to substitute a different biological under the new National Health (Pharmaceutical Benefits) (Pharmacist Substitution of Medicines without Prescription during Shortages) Determination 2021. The term ‘substitution’ is a multivalent term in Australia, contained in the National Health Act 1953 and refers to the practice of dispensing. This designation was first applied to biosimilars within the PBS with the introduction of the etanercept biosimilar, followed by adalimumab [4]. Enabling pharmacists to decide which biosimilars and/or originator to dispense has created an interesting dynamic. Some clinicians who prescribe biologicals are not accepting of this approach in part or in whole [3, 5]. As a result of their concerns, some clinicians have taken the step of indicating ‘substitution not permitted’ on the prescription, effectively preventing the pharmacist from substituting a biosimilar for the originator. In recent time, some peak medical bodies in Australia have supported the use of biosimilars, recognizing that biosimilar medicines can be expected to deliver the same clinical outcomes for patients and at a lower cost [6]. Further hampering the uptake of biosimilars in Australia is the manner in which ‘substitution’ of biosimilars has been implemented. The Australian Government has indicated that they are in favour of pharmacists substituting biosimilars [7] but have also indicated that the prescribers have the final word on this and can block this action using the ‘substitution not permitted’ designation on the prescription. So where does this leave Australia? Three viable options exist:
Clinicians allow the pharmacist to substitute the product to a biosimilar, across biosimilars, or back to the reference medicine.
Clinicians indicate ‘Substitution Not Permitted’ on prescription and pharmacists are not allowed to substitute.
Clinicians and pharmacists develop collaborative relationships and communicate clearly with each other the boundaries, clinical goals, appropriate approaches to biosimilar substitution, and where substitution may or may not be appropriate.
We assert here that the preferable approach is the latter. While this may require more substantial efforts to develop and manage these relationships, it is the approach that will most likely lead to long-term success with biosimilars and is in concordance (but an extension to) with the current Australian Government Biosimilar Awareness Initiative.
While there are no specific roadmaps for opening these clinician-pharmacist conversations about biosimilars, the first step is to pick up the phone or strike up a conversation, and to maintain a co-operative approach. Each conversation between pharmacists and clinicians, the boundaries they set, and the ways of cooperating will differ. However, foundational to each conversation should be that biosimilars are safe and effective and will be critical to reducing healthcare system cost burdens when used appropriately and in co-operative agreement between patients, clinicians, and pharmacists, in concordance with both Australia’s Quality Use of Medicines and Medicines Safety policy on medication safety.
Competing interests: None for Lisa Hall and David Lim. Chad Rieger is the Medical Manager of Biosimilars with Sandoz. Chad is not paid for his involvement in the manuscript. Neither Lisa nor David was paid for their involvement in the manuscript. Chad’s involvement in the manuscript was in his private and personal capacity as PhD candidate with The University of Queensland.
Provenance and peer review: Not commissioned; internally peer reviewed.
Authors
Chad Rieger1, MBA Lisa Hall1, PhD David Lim2, 3, DPH
1.School of Public Health, Faculty of Medicine, The University of Queensland 2.Translational Health Research Institute, School of Health Sciences, Western Sydney University 3.College of Medicine and Public Health, Flinders University
References 1. Lim D, Bandiera R, Handsley E. Switching Australian patients with moderate to severe inflammatory bowel disease from originator to biosimilar infliximab. Med J Aust. 2021;215(9):435 doi:10.5694/maj2.51295 2. Bandiera R, Handsley E, Lim D. Born with a plastic spoon in their mouth? – Substitution, interchangeability, and marketing of biosimilars. J Law Med. 2022;29(1):208-23. 3. Lau E, Lim D, Baldry R, Nissen L. What drug: biosimilars. Aust J Pharm. 2016;35(3):64-6. [homepage on the Internet]. [cited 2022 Jul 4]. Available from: https://search.informit.org/doi/abs/10.3316/informit.295852761863296 4. Australian Government. The Pharmaceutical Benefits Scheme. 25 June 2022. Considering brand equivalence/substitution for biosimilar medicines [homepage on the Internet]. [cited 2022 Jul 4]. Available from: https://www.pbs.gov.au/industry/listing/elements/pbac-meetings/psd/2018-03/files/biosimilar-medicines-considering-brand-equivalence-substitution-psd-march-2018.pdf 5. Lim D. Is Australia positioned to take advantage of biosimilars? Generics and Biosimilars Initiative Journal (GaBI Journal). 2014;3(4):184-7. doi: 10.5639/gabij.2014.0304.042 6. Gregory GP, Carrington C, Cheah CY, Hakes EA, Irving IM, Siderov J, et al. A consensus statement on the use of biosimilar medicines in hematology in Australia. Asia Pacific J Clin Oncol. 2020;16(4):211-21. 7. Australian Government. The Pharmaceutical Benefits Scheme. 25 June 2022. Biosimilar uptake drivers [homepage on the Internet]. [cited 2022 Jul 4]. Available from: https://www.pbs.gov.au/general/biosimilars/biosimilar-uptake-drivers-q-and-a.pdf
Author for correspondence: David Lim, DPH, Western Sydney University, Locked Bag 1797, Penrith, NSW 2751, Australia
Disclosure of Conflict of Interest Statement is available upon request.
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Author byline as per print journal: Federico J Piñeiro, Pharm, MPH; Fernández Argüelles Rogelio Alberto, Pharm, PhD
Introduction/Objective: To describe the chiral switch, an evergreening strategy used by AstraZeneca to position enantiopure esomeprazole as the new proton pump inhibitor market leader, displacing its predecessor omeprazole. Methodology: A four-stage systematic review which included: a preliminary review, bibliographic review using databases, classification of the body of literature, and content analysis. Results: Using different legal and commercial strategies, such as patent thickets and aggressive publicity campaigns, AstraZeneca transferred consumer loyalty from their successful omeprazole to esomeprazole, its new and more expensive patent protected product which has the same therapeutic value as its predecessor. This chiral switch allowed AstraZeneca to maintain monopoly prices, which increased the financial burden experienced by consumers and payors and may have also had a negative impact on access to the medication. Conclusions: This case study exemplifies how the current patent system, including patent thickets, can be used to enhance the profits of pharmaceutical companies while stalling innovation and placing undue financial burdens on the consumer.
Submitted: 18 December 2021; Revised: 2 May 2022; Accepted: 6 May 2022; Published online first: 20 May 2022
Introduction/Objective
The 20th century witnessed extraordinary medical advances that have eradicated or controlled epidemics across the world and have lessened the impact of life-threatening diseases. Undeniably, the widespread use of pharmaceuticals has contributed to the sustained increase in life expectancy observed throughout this period. The pharmaceutical industry’s investments in research and development (R & D) have resulted in major contributions to our therapeutic arsenal. However, since Arnold Relman published ‘The new medical-industrial complex’ [1], significant changes in the business model adopted by the major pharmaceutical companies (from now on ‘Big Pharma companies’) have been observed [2].
Under the new paradigm, these companies, which trade in the stock market and must respond to the interests of the stockholders, no longer prioritize the development of drugs that would add high therapeutic value, but rather those that would maximize their profits [3]. To achieve this goal, in the context of the emergence of generic drugs in the late 1980s and 1990s, Big Pharma started focusing on maintaining the high prices facilitated by monopolies and worked on extending the commercial exclusivity of brand-name drugs. In other words, the industry maximized profits by using incentives intended to reward innovation to instead maximize their profits. These are outlined in Table 1 and include the protection of intellectual property through patents and data exclusivity.
The term ‘evergreening’ refers to the use of legal, commercial and technological strategies to extend due-to-expire patents of successful products [6-8]. Big Pharma companies have used evergreening to prolong their legal monopoly, enabling the patent owner to maintain high prices and avoid losing the commercial benefits that would likely result from the commercialization of generic versions of their branded products [9, 10].
To shield the power of their monopoly, Big Pharma companies use evergreening and other strategies, such as taking advantage of aspects of legislation, to delay the entry of generics. For example, in the United States (US), the Hatch-Waxman act, extends the market exclusivity period of a new drug by six months when clinical trials are carried out in a paediatric population [11, 12], even if that drug does not treat a medical condition that occurs in paediatric patients.
Moreover, many Big Pharma companies have been increasingly developing drugs that are very similar to their original products (the so-called ‘me-too or follow-on drugs’). These are then launched just before the expiration of the patent on their original drug. When these drugs are released into the market, they are intensively promoted as being more advantageous than predecessors [7, 12, 13]. These new drugs can be developed using different shunting maneuvers, see Table 2, including the following: commercializing the active enantiomer of a drug already on the market (this ‘chiral switch’ strategy is described in detail below), modifying the formulation of the active pharmaceutical ingredient (API), using the active metabolite of a previously commercialized product, and combining more than one API in the same presentation.
Most drugs that contain a chiral centre are marketed as racemic mixtures, that is, a combination of the two possible enantiomers. Usually, these two ‘halves’ have similar clinical activity and adverse effects; however, sometimes a pure enantiomer – also called enantiopure – may offer some therapeutic advantages. The market launch of an enantiopure product just before the patent expiration of its racemic predecessor has been described as a ‘chiral switch’ strategy, and often the new product does not offer any clinical advantages to justify the change [13, 14].
A relevant example of a chiral switch is the case of AstraZeneca’s omeprazole/esomeprazole. In 2000, omeprazole the lead proton-pump inhibitor (PPI), was the world’s bestseller, with annual US sales of US$6 billion a year, under the brand name Prilosec [15]. However, by 2010, enantiopure esomeprazole (sold as Nexium) became AstraZenca’s bestseller with US sales of US$5.63 billion, compensating for the plummeting of omeprazole [16]. According to Coherent Market Insights, in 2020 the estimated value of the global PPI market was US$2.9 billion and it was expected that its compound annual growth rate (CAGR) would be 4.30% during 2020–2027. The success in launching esomeprazole allowed AstraZeneca to maintain its leadership in the PPI market.
The objective of this article is to describe the omeprazole/esomeprazole chiral switch used by AstraZeneca as a case study that exemplifies the behaviours of the pharmaceutical industry. More specifically, we will analyse the published literature on the clinical evidence of esomeprazole’s therapeutic value and how AstraZeneca took advantage of regulations and pricing mechanisms to position enantiopure esomeprazole into a dominant market position.
Methodology
A qualitative systematic review was carried out in four stages. Initially, in the exploratory stage, the pre-existing knowledge and the theoretical framework were outlined. Subsequently, a literature search was carried out, using the digital databases: Scientific Electronic Library Online (SciELO), Scopus, Virtual Health Library (VHL), Sistema de Información Esencial en Terapéutica y Salud (SIETES) and PubMed. The goal was to generate a representative body of literature covering a wide geographic range and incorporating different approaches and opinions.
All searches, except SIETES, were done in English, using the terms: ‘blockbuster’, ‘pharmaceutical industry’, ‘esomeprazole’, ‘omeprazole’, ‘big pharma’, ‘patents’ and ‘evergreening’. In SIETES, due to the modality of this database, the search was carried out using the following Spanish keywords: ‘esomeprazol’, ‘patentes’, ‘enantiomeros’ and ‘industria farmacéutica’. Table 3 includes more details on the bibliographic search and the absolute number of articles identified through each search engine. Only peer-reviewed, scientific articles written in English, Spanish or Portuguese were included.
The references of all the included articles were reviewed to identify additional references and other technical reports suggested by experts were incorporated into the analysis. After removing duplicate articles and those that did not meet the inclusion criteria, 32 of the 167 articles that had been identified were selected for analysis.
In the third stage, the body of articles were classified using content analysis techniques, particularly thematic analysis [17].
Results
Thirty-two articles were included in the final analysis and these were mostly written by researchers from Europe, the US and Australia. The information contained in the articles was classified into three different categories: clinical, regulatory and commercial.
Clinical aspects Esomeprazole, the S-isomer of omeprazole, was launched in the US market by AstraZeneca, under the name Nexium® in 2001, a few months before the expiration of patent of omeprazole (Prilosec®). The loss of the omeprazole patent threatened the financial position of the company as it was their global bestseller [1, 15].
Given that omeprazole and esomeprazole have the same chemical structure and do not present pharmacodynamic differences, the company justified the development of the enantiopure exclusively on pharmacokinetic differences, particularly a difference in the affinity for CYP2C19, an enzyme belonging to the large hepatic enzyme complex of cytochrome P450, whose basic function is to transform its substrates into more polar and soluble molecules, thus facilitating their excretion. This would result in esomeprazole remaining active for a longer period than omeprazole [6].
In terms of published evidence, several studies [14, 18–20] have shown that the pivotal clinical trials of esomeprazole compared its efficacy against omeprazole at non-equipotent doses, and some trials used placebo as a comparator. Likewise, not all the results were favourable for the new enantiomer, and two articles [14, 18] unveiled the presence of publication bias. While the articles that showed the advantages of the new drug were published in the same year as its market approval, the studies that did not show a significant difference between the two drugs were published five years after approval when the new drug had already established itself as the best option to treat heartburn.
Regulatory aspects Given the commercial importance of omeprazole, AstraZeneca deployed a wide variety of regulatory strategies to maintain its monopoly, as discussed in the following paragraphs.
Secondary patents: there are two types of patents; primary patents, which protect new chemical or biological compounds intended for therapeutic use in humans; and secondary patents, which protect non-essential aspects of the new molecule, such as small chemical variants, different crystalline conformations of the original compound, methods of use, new formulations and new dosage forms [8, 21].
A 2010 analysis of the Food and Drug Administration (FDA) website found that, in the US, omeprazole was protected by a total of 40 patents [22], constituting a ‘patent thicket’. Another example of such a thicket is highlighted in an article on the Australian market [23] which asserts that, in addition to the original patent for omeprazole, there were 61 additional patents, two of which clearly appear to have prevented generics from entering the market. Initially, an enteric-coated formulation, developed to delay the absorption of the active principle, precluded the commercialization of generics between 1999 and 2006, a period during which a new patent was introduced for the enantiomer esomeprazole [23, 24]. Taking the exclusivity period granted for the new product into account, the effective market monopoly of these two drugs (omeprazole and esomeprazole) in Australia exceeds 29 years [23].
Litigation for patent usurpation: Patent thickets are often used by Big Pharma to enable them to sue generic companies that attempt to enter the market; the greater the number of patents, the easier it is for Big Pharma to claim that one of them has been violated. The litigation process allows Big Pharma companies to extend their commercial exclusivity by the period noted in the legislation. For example, in the US, FDA-approved drugs and all their patents are included in the so-called ‘Orange-Book’, and when a generics manufacturer wants to market a generic of a brand-name drug it must submit an abbreviated new drug application (ANDA) to FDA. In addition, to ensure that no patent is being infringed, the generics manufacturer must certify one of the following:
i) the drug has not been patented ii) the patent has already expired iii) the generic drug will not enter the market until the patent expires iv) the patent is invalid or will not be infringed by the generic drug.
If the fourth option is chosen (called ‘paragraph IV certification’), a notice must be sent immediately to the patent holder, who will have 45 days to take the case to court on the basis that the generic drug infringes a patent listed in the Orange Book. If the branded drug producer decides to litigate, the generic drug approval will automatically be delayed for 30 months or until the dispute is resolved or the patent expires, whichever occurs first [18].
Generics manufacturers, who are generally smaller and have fewer financial resources, are often discouraged by the high costs of the legal process. They face the dilemma of having to choose between entering the legal dispute, assuming the costs and the risk of an unfavourable resolution, or simply postpone their market entry until being absolutely sure that both primary and secondary patents have expired.
Paediatric clinical trials: Using federal regulations, AstraZeneca conducted paediatric clinical trials with omeprazole in the US, obtaining an additional six months of market exclusivity [1, 18].
Switching prescription drugs to over-the-counter (OTC): According to Kakkar (2015), AstraZeneca imposed a ‘double switch’ in the US: the chiral switch of Nexium, and the subsequent switch of Prilosec from prescription to OTC, shortly afterwards. Another article reports the use of the same strategy in Sweden, where, in 1999, the company also requested the change of omeprazole from a prescription to an OTC drug [25].
Commercial aspects Several authors agree that AstraZeneca’s chiral switch was accompanied by an aggressive publicity campaign to encourage loyal consumers of the original racemic mixture to use the new patent-protected enantiopure product [26, 27]. In the US alone, it invested US$500 million, in direct advertising to the consumer, medical samples and discounts offered to hospitals when using the new drug [18, 28]. The US advertising campaign appears to have been successful as, shown in Figure 1, shortly after launching Nexium, its sales exceeded those of its predecessor.
Another article analysed the PPI market in Australia and highlighted that in 2003, of all prescriptions for the omeprazole/esomeprazole binomial, only 18% were for the new drug, while omeprazole retained the remaining 82%. By 2014, this proportion was inverted, and esomeprazole accounted for 77%, while omeprazole only held 23% [23].
A 2013 study [6] of the US market calculated the price difference between an equipotent dose of these two drugs for six weeks of treatment and found that patients using esomeprazole spent US$111 more that those using omeprozale. It is estimated in just a year, AstraZeneca generated an additional US$1.5 million from this chiral switch. Another article claims that 40% of patients in the US had switched to the new drug in 2003, and that change represented company earnings of US$3 billion during that year, and at least US$5 billion in 2004 [29]. In 2009, in England, the National Health Service (NHS) spent £42 million on esomeprazole at the primary healthcare level, despite the fact that it offers no clinical advantages and is 11 times more expensive than other available PPIs [30]. Similarly, an article that studied the costs associated with eight ‘follow-on drugs’ in Geneva, Switzerland found that the most prescribed was esomeprazole (55% of the total), which represented an additional cost of €5.2 million over the cost of using generic omeprazole during the period studied (2000‒2008) [31].
In 2003 in Australia, shortly after its approval, the price of esomeprazole was 118% that of omeprazole. This continued to increase and, in 2014, it had become 200% more expensive [23], see Figure 2.
Discussion
The results show the success of the strategies used by AstraZeneca to switch consumer loyalty from the successful omeprazole to the new esomeprazole, which allowed the company to maintain high monopoly prices. This case study also highlights the inability of the current intellectual property protection system to guarantee universal access to pharmaceuticals at affordable prices. This failure is reflected in the three interrelated issues that are discussed below.
Patent thickets The patent system was designed so that, after a period of exclusivity, competing companies could develop and market the same product, engendering competition and leading to lower prices, while the period of intellectual property protection would serve as an incentive for Big Pharma to continue to invest in R & D [32]. However, in the case of pharmaceutical products, the reality is usually quite far from this theoretical model.
Patent authorities often award patents for trivial changes, and Big Pharma companies are using this to their advantage and often succeed in avoiding the commercial losses that would ensue from the presence of competing generics. In some European countries, the price of generics could be as low as 2% to 4% of the originator’s price before patent expiration [33], therefore, most innovative companies stand to lose a large share of their markets with the introduction of generics and therefore use a combination of strategies to maintain profits. In relation to this, a recent article points out that in the US, the popular etanercept is still under patent protection 37 years after its first patent was issued and 17 years after the main patent expired [32]. These patent thickets enable companies to maintain their market exclusivity, set high prices, and even expand their market share.
In the last two decades, the patent thicket practice has become widespread. Feldman (2018) shows that according to FDA’s records, between 2005 and 2015, 78% of the new patents were not issued for newly developed chemical compounds, but for changes made to some characteristics and/or manufacturing processes of drugs that were already in the market. Moreover, in the US, the ratio between secondary patents and primary patents has recently reached 7 to 1 [33]. These low-quality patents have been questioned in various countries because they might not meet patentability requirements (novelty, non-obviousness and industrial applicability), and have led to an increase in the litigation of intellectual property infringements [34]. The trick consists of protecting the original products with multiple patents to increase the possibilities that the release of a generic version might infringe a patent, lead to litigation and delay the presence of competing products.
This would not be a serious problem if it were not closely related to the fact that the low level of required inventiveness to grant patents, discourages real innovation while maintaining monopoly prices.
In the case of AstraZeneca’s chiral switch, the company wanted to maintain its leadership in the PPI market, so is not surprising that it was willing to use anti-competitive tactics, for which it has subsequently had to pay fines and defend its patents in court [15, 35].
Lack of innovation If companies can extend their commercial monopolies without the need to strive for true innovation, it is not surprising that most newly commercialized drugs offer few additional benefits over older medicines. The increasing interest in enantiopure drugs seems to come in response to this way of thinking. Using data from the independent French publication Prescrire as a reference, of the 92 new products and indications that were approved in 2016, only 15 (or 16%) represented a possible therapeutic advance. These data do not appear to be exclusive to 2016 as the number of true innovative products has not changed much in the last 10 years [36].
Big Pharma’s R & D is focused on resolving problems that affect a large number of patients who can pay for drugs [1]. So, the lack of innovation is even more pronounced for diseases that affect fewer people and these become neglected. Only 4% of the drugs approved by FDA and the European Medicines Agency (EMA) between 2000 and 2011 were intended for the treatment of such pathologies [37]. Given that most of these neglected diseases are concentrated in developing countries [38], it is reasonable to think that the responses that Big Pharma is offering to these countries is even less satisfactory.
High prices Although patients’ access to drugs depends on various factors, price is undoubtedly a key factor and high prices are a major public concern that threaten the medium-term viability of the health systems.
It should be noted that, according to the innovative pharmaceutical industry, prices do not only reflect the cost of raw materials, manufacturing and advertising of the approved product, but also the investment in R & D of products that have failed. However, the lack of transparency in Big Pharma’s expenditures precludes observers from verifying if the prices are linked to reasonable expenditures on each of these components [39]. Critics have suggested that these industries engage in other behaviours that lead to excessive pricing, such as providing high returns to investors, offering attractive compensation packages for senior executives, paying fines due to regulatory violations, extensive lobbying activities, and being involved in mergers and acquisitions above market value [40–42].
Published data show that governments, health insurers and patients in the US, Europe and Australia increased their expenditures on PPIs after esomeprazole became available in those countries.
Moir’s results (2016) appear to support the use of ‘shadow pricing’, a concept proposed by Angell [1], referring to the fact that companies usually set the price of a new drug in a range very similar to that of its predecessor (or in some cases, lower), in order to favour the transition to the new drug. Subsequently, once various generic drugs have entered the market, competition usually reduces the price of the original drug, increasing the price gap with the successor that is still under patent.
The problem with high prices is that many populations are left behind and without access to life-saving drugs. It is widely demonstrated in the literature [43, 44] that commercialization of generics promotes competition and lowers prices. In the case presented, an aggressive marketing campaign and patent thickets allowed a monopoly to be extended, which was detrimental to patients’ interests.
Together, these strategies have many consequences for patients, insurance companies and healthcare institutions. This manuscript has attempted to shed light on the problem and to encourage the implementation of independent cost-effectiveness studies. The comparison of all available therapeutic options could lead to better treatment choices, better health outcomes and the improved use of available resources.
Strengths and limitations This manuscript’s main strength is that it has systematically and qualitatively evaluated the published literature surrounding AstraZeneca’s chiral switch omeprazole/esomeprazole. It has also systematically scrutinized the strategies used by AstraZeneca to extend its commercial monopoly in different countries.
The manuscript also has some limitations, being a qualitative systematic review, the use of search terms and the selection of articles is always affected by the subjective decision of the authors. Therefore, although the choice of databases and search terms was aimed at generating a representative body of literature, some relevant articles may have been omitted. Furthermore, the inclusion of additional chiral switch case studies could yield additional information on how new enantiopure substances have entered the market, in some cases such products may have provided clinical benefits to patients.
Conclusion
AstraZeneca’s omeprazole/esomeprazole chiral switch evergreening strategy was used to extend the commercial exclusivity of their blockbuster drug product. They introduced the enantiopure esomeprazole to the market as a new product, although it had no clinical advantages over its predecessor, omeprazole. As mentioned previously, this case was chosen due to the size of the PPI market and because it exemplifies the way in which the company deployed different strategies to prolong commercial exclusivity and increase its profits. This led to an increase in drug spending, both for individuals and for the public health systems.
Our continued reliance on Big Pharma companies for drug R & D and production has resulted in markets flooded with products with little or no utility, that often do not respond to the actual needs of the population.
This study has outlined three major problems that have resulted from the failures of the patent system and how they are closely related. The case of omeprazole/esomeprazole is paradigmatic; it shows that Big Pharma’s main goal is no longer the development of drugs with therapeutic value, but one of pseudo-innovation to maintain commercial monopolies for extended periods. This business model aims at maximizing profitability and not at preventing or curing diseases. Unless changes are promoted in the institutions responsible for guaranteeing intellectual property protections in the different countries, the granting of low-quality patents will continue to result in prolonging monopolies and discouraging true therapeutic innovation.
The study highlights that the current patent system is inefficient and does not work to benefit patients. It is therefore imperative to strengthen knowledge and competence at all levels of the healthcare systems to enhance the use of the most cost-effective medical options. It is also important to promote mechanisms to orient the R & D of the pharmaceutical sector towards medicines that respond to the health needs of the population and not to the interests of Big Pharma. Alternative models are being proposed, including public R & D, innovation prizes, and governmental investments in new products that are later sold by private companies with a reasonable profit margin. It is important to invest in exploring these and other alternative paths, to improve access to medicines in all regions of the world and prevent access to medicines being a privilege only for the few.
Summary paragraph: The authors believe the information contained in this manuscript may be relevant for prescribers, patients and the community in general. All of them will benefit from learning about the strategies used by the pharmaceutical industry that lead to increased prices for prescription drugs.
Acknowledgements
We would like to express our very great appreciation to Nuria Homedes, for her valuable and constructive suggestions to improve this research work.
Competing interests: The authors declare that there is no conflict of interest. This work has been carried out thanks to a CONICET (Argentina) scholarship. Provenance and peer review: Not commissioned; externally peer reviewed.
Authors
Federico J Piñeiro, Pharm, MPH Instituto de Salud Colectiva, Universidad Nacional de Lanús, 309 Thames, 1414 Buenos Aires, Argentina
Fernández Argüelles Rogelio Alberto, Pharm, PhD Universidad Autónoma de Nayarit, 56 Shangay, Colonia Insurgentes, 63183 Tepic. Nayarit, México
References 1. Relman AS. The new medical-industrial complex.N Engl J Med. 1980;303(17): 963-70. 2. Angell M, Freire L. La verdad acerca de la industria farmacéutica cómo nos engaña y qué hacer al respecto. Bogotá: Grupo Editorial Norma; 2006. 3. Ugalde A, Homedes N. Medicamentos para lucrar. La transformación de la industria farmacéutica. Salud Colectiva. 2009;5(3):305-22. 4. Allard Soto R. Medicamentos esenciales y acuerdo sobre los ADPIC: colisión entre el derecho a la salud y el derecho de propiedad intelectual. Salud Colectiva. 2015;11(1):9-21. 5. Musungu SF, Villanueva S, Blasetti R. Utilizing TRIPS flexibilities for public health protection through South-South regional frameworks. 2004. CiteSeerX. [homepage on the Internet]. [cited 2022 May 2]. Available from: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.297.6970&rep=rep1&type=pdf 6. Lehmann DF, Wojnowicz S. The evergreening of biopharmaceuticals: time to defoliate. J Clin Pharmacol. 2016;56(4):383-9. 7. Feldman R. May your drug price be evergreen. J Law Biosci. 2018;5(3):590-647. 8. Collier R. Drug patents: the evergreening problem. CMAJ. 2013;185(9):E385-6. 9. Kesselheim AS. Rising health care costs and life-cycle management in the pharmaceutical market. PLoS Med. 2013;10(6):e1001461. 10. Kesselheim AS, Avorn J, Sarpatwari A. The high cost of prescription drugs in the United States: origins and prospects for reform. JAMA. 2016;316(8):858-71. 11. Darrow JJ, Avorn J, Kesselheim AS. FDA approval and regulation of pharmaceuticals, 1983-2018. JAMA. 2020;323(2):164-76. 12. Christie AF, Dent C, McIntyre P, Wilson L, Studdert DM. Patents associated with high-cost drugs in Australia. PLoS One. 2013;8(4):e60812. 13. Kakkar AK. Patent cliff mitigation strategies: giving new life to blockbusters. Expert Opin Ther Pat. 2015;25(12):1353-9. 14. Gellad WF, Choi P, Mizah M, Good CB, Kesselheim AS. Assessing the chiral switch: approval and use of single-enantiomer drugs, 2001 to 2011. Am J Manag Care. 2014;20(3):e90-7. 15. Hawkes N. AstraZeneca must pay €52.5m fine for anticompetitive tactics, rules European court. BMJ. 2012;345:e8396. 16. Lindsley CW. The top prescription drugs of 2012 globally: biologics dominate, but small molecule CNS drugs hold on to top spots. ACS Chem Neurosci. 2013;4(6):905-7. 17. Souza Minayo ME. La artesanía de la investigación cualitativa. 1°. Buenos Aires: 2013. 18. Dwivedi G, Hallihosur S, Rangan L. Evergreening: a deceptive device in patent rights. Technol Soc. 2010;32(4):324-30. 19. Gilhooley M. Heal the damage: prescription drug consumer advertisements and relative choices. J Health Law. 2005;38(1):1-44. 20. Shivashankar M, Mani D, Mandal BK. An overview on intellecual property rights in pharmaceutical and biotechnology industries. J Chem Pharm Res. 2011;3(2):753-61. 21. Organización Mundial de la Propiedad Intelectual. Resumen del estudio sobre patentes farmacéuticas en Chile. 2015 [homepage on the Internet]. [cited 2022 May 2]. Available from: https://www.wipo.int/edocs/mdocs/mdocs/es/cdip_15/cdip_15_inf_2.pdf 22. Lourenço AL, Lira LM, Carvalho DP de, Melo P de A, Cláudio-da-Silva TS. Gestão das inovações incrementais, o caso Omeprazola. Química Nova. 2010;33(4):1000-4. 23. Moir H. Exploring evergreening: insights from two medicines. Aust Econ Rev. 2016;49(4):413-31. 24. Lloyd M. Evergreening by whom? A review of secondary patents for omeprazole. Pharm Pat Anal. 2013;2(6):737-43. 25. Cohen JP, Paquette C, Cairns CP. Switching prescription drugs to over the counter. BMJ. 2005;330(7481):39-41. 26. Kyle GJ, Nissen LM, Tett SE. The Australian rise of esomeprazole-was expenditure on samples a contributor? Pharmacoepidemiol Drug Saf. 2009; 18(1):62-8. 27. Somogyi AA, Bochner F, Foster D. Inside the isomers: the tale of chiral switches. Aust Prescr. 2004;27(2):47-49+51. 28. Hess J, Litalien S. Battle for the market: branded drug companies’ secret weapons generic drug makers must know. J Generic Med. 2005;3(1):20-9. 29. Dutfield G. Healthcare innovation and patent law’s ‘pharmaceutical privilege’: Is there a pharmaceutical privilege? And if so, should we remove it? Health Econ Policy Law. 2017;12(4):453-70. 30. Hughes DA, Ferner RE. New drugs for old: disinvestment and NICE. BMJ. 2010;340:c572. 31. Vernaz N, Haller G, Girardin F, Huttner B, Combescure C, Dayer P, et al. Patented drug extension strategies on healthcare spending: a cost-evaluation analysis. PLoS Med. 2013;10(6):e1001460. 32. Gardner J. A three-decade monopoly: how Amgen built a patent thicket around its top-selling drug. Biopharma Dive. 2021 November 1. 33. Song CH, Han J-W. Patent cliff and strategic switch: exploring strategic design possibilities in the pharmaceutical industry. SpringerPlus. 2016;5(1):692. 34. Martínez Pérez M. Las patentes sobre “second generation products” utilizadas como estrategia para dilatar la entrada de genéricos en el mercado de la Unión Europea. Cuadernos de Derecho Transnacional. 2014;6(2):175-200. 35. Owens J. EC fines AstraZeneca in Losec antitrust case. Nat Rev Drug Discov. 2005;4(7):530. 36. New products and new indications in 2016: a system that favours imitation over the pursuit of real progress. Prescrire Int. 2017;26(182):136-9. 37. Pedrique B, Strub-Wourgaft N, Some C, Olliaro P, Trouiller P, Ford N, et al. The drug and vaccine landscape for neglected diseases (2000–11): a systematic assessment. Lancet Glob Health. 2013;1(6):e371-9. 38. Kindhauser MK. Communicable diseases 2002. Global defence against the infectious disease threat. Geneve: World Health Organization; 2003. 39. Perehudoff K, Mara K, ‘t Hoen E. What is the evidence on legal measures to improve the transparency of markets for medicines, vaccines and other health products (World Health Assembly resolution WHA72.8)? Copenhagen: WHO Regional Office for Europe; 2021. PMID: 34351727. 40. Light DW, Warburton R. Demythologizing the high costs of pharmaceutical research. BioSocieties. 2011;1:34-50. 41. Drug research: public funding, private profits. Prescrire International. 2020; 29(221):303-6. 42. Brown D, Hanna TH. It’s time for a public option in the pharmaceutical industry. In TheseTimes. 11 May 2018. [cited 2022 May 2]. Available from: https://inthesetimes.com/article/pharmaceutical-industry-drug-prices-trump-public-option 43. Simoens S. A review of generic medicine pricing in Europe. Generics and Biosimilars Initiative Journal (GaBI Journal). 2012;1(1):8-12. doi:10.5639/gabij.2012.0101.004 44. U.S. Food and Drug Administration. Generic competition and drug prices: new evidence linking greater generic competition and lower generic drug prices. 2019 [homepage on the Internet]. [cited 2022 May 2]. Available from: https://www.fda.gov/media/133509/download
Author for correspondence: Federico J Piñeiro, Pharm, MPH, Instituto de Salud Colectiva, Universidad Nacional de Lanús, 309 Thames, 1414 Buenos Aires, Argentina
Disclosure of Conflict of Interest Statement is available upon request.
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
Author byline as per print journal: Adjunct Associate Professor Sia Chong Hock, BSc (Pharm), MSc; Christine Koh, BSc (Pharm) (Hon); Associate Professor Chan Lai Wah, BSc (Pharm) (Hon), PhD
Abstract:
Cell, tissue and gene therapy products (CTGTPs) are therapeutic products intended for use in humans for prophylactic, diagnostic, curative, palliative or diagnostic purposes. Generally, they are breakthrough therapies with immense potential in treating diseases with no cure or rare diseases with high treatment burdens. Thus far, the number of approved cell, tissue and gene therapies globally are few and far between, with some approved products being recalled due to safety and efficacy issues. This situation highlights the need to rectify the challenges that are present in the manufacturing and regulation of these medicines. This article presents an overview of how CTGTPs work using examples of existing approved products across different product categories, as their mechanisms of action and characteristics contribute to manufacturing challenges. The differences between CTGTPs and conventional biologicals will be highlighted to understand the need for different regulatory frameworks to be designed. Additionally, these frameworks by the major regulatory authorities and international organizations will be analysed to elucidate whether CTGTPs are regulated to different extents across countries. Challenges faced in the manufacturing and regulation of CTGTPs include quality assurance issues, lack of expertise and limitations in technology. Potential solutions include implementing a tighter regulatory framework, fostering the international harmonization of regulations, increasing outsourcing to meet good manufacturing practice (GMP) guidelines, and incorporating automation into manufacturing processes to improve quality control to address the challenges encountered.
Submitted: 29 January 2022 Revised: 11 March 2022; Accepted: 14 March 2022; Published online first: 28 March 2022
Introduction
Cell, tissue and gene therapy products (CTGTPs) are distinct categories of therapeutic products intended for use in humans for curative, prophylactic, palliative or diagnostic purposes [1]. Currently, these revolutionary products target diseases that are managed by therapies with high treatment burdens such as the use of recombinant factor IX protein therapy in lieu of repeated intravenous blood infusions for haemophilia B, or rare genetic diseases where no therapies exist for patients, as in Friedreich’s ataxia FRDA) [2].
Cell therapies include the use of stem cells for regenerative purposes [3], or via the insertion of gene for special receptors such as the chimeric antigen receptor (CAR) onto T-cells, as gene therapies for the treatment of cancers and rare diseases. Gene therapies offer a more permanent solution to genetic diseases, when compared to conventional treatments such as chemotherapy through the introduction of genetic material which produces therapeutic proteins [4]. Typically, this circumvents the restrictions related to the therapeutic use of recombinant peptides, including low bioavailability, clearance rates, and exorbitant production cost [5]. Tissue therapies aim to mend and restore injury to organs and tissues through the engineering of components involving cells and tissue architectures [6], combining cells from a patient with scaffold biomaterials [7], which can potentially plug the severe shortage in donated organs. Currently, there are over a hundred thousand potential recipients on the waiting list in the United States alone [8].
CTGTPs have been defined and classified differently by various regulatory bodies, where a product will go through the regulatory pathway according to the definition that they fall under. In some countries, CTGTPs are also known as advanced therapy medicinal products (ATMPs) or regenerative medicines (RM). In other countries, they may be further classified under categories such as cell therapy medicines, gene therapy medicines, tissue-engineered medicines, or combined products, with different variations in naming the respective product categories. These definitions take into consideration the degree of processing from the starting materials as well as the purpose of the product, such as the restoration of function or prevention of disease, which determines the extent of regulation a product is subject to. However, there are also some countries where little or no regulations for CTGTPs exist.
With rapid progress and strong interest in CTGTPs, as evident from the increase in investments in these novel products over the last decade [7], many challenges have also arisen. These come from a lack of knowledge regarding these novel products, where conventional modes of manufacturing and regulation have not been adequately adapted to ensure the safety and efficacy of CTGTPs. Considering the lack of studies on CTGTPs, this article aims to juxtapose the characteristics of CTGTPs with conventional biologicals, where existing manufacturing trends from the latter will serve as a basis for proposing solutions to solve the challenges faced in manufacturing and regulation. This article also aims to present the manufacturing processes and regulatory frameworks that CTGTPs are subjected to in different countries.
CTGTPs and their principles of action
Cell therapy products use cells to repair or replace injured tissue or cells in the body. Cells used may include mesenchymal stem cells (MSCs), T cells, and pancreatic islet cells [9]. Cell therapy products may contain only cells alone or exist as a part of gene therapy or tissue therapy.
These products can be further categorized according to autologous therapies or allogeneic therapies. Autologous therapies obtain cells directly from the patient, thus circumventing immune reactions. However, this also means that these cells are not suitable for use in mass manufacturing as ‘off-the-shelf’ products. In contrast, allogeneic therapies utilize donated cells to treat multiple patients. These cells are collected from healthy donors, rather than directly from the patient to create a master cell bank (MCB). Consequently, the risk of immunogenic reactions is higher [16]. Products for gene therapies are manufactured via ex vivo or in vivo processes. An in vivo process is one where a viral vector carrying the gene of interest is directly transferred into the body via infusions, whereas an ex vivo process involves removing a patient’s cells to be altered and then re-infusing the genetically modified cells back into the patient’s body [17]. For tissue engineering, current strategies include recreating organ and tissue structure via scaffold fabrication, 3D bioprinting and self-assembly, integration of grafts to host via vascularisation and changing the host environment to create therapeutic responses [6].
Regulators often decide on the stringency of manufacturing requirements by considering if the therapy product is intended for homologous use, where the therapy product is administered at an identical anatomical site and fulfils the same function in the recipient as in the donor [1]. In addition, the extent of manipulation the cells or tissues have undergone is also considered, where minimal manipulation implies that biological traits or functions of the cell or tissue are unchanged [1].
Differences between CTGTPs and conventional biologicals
The type of therapy has an immense impact on the type of manufacturing style and challenges encountered. Conventional biologicals are biotherapeutic protein products made with recombinant DNA technology, where cells are reprogrammed genetically to produce proteins that are insufficiently produced in the body [10]. An example includes synthetic insulin for the treatment of diabetes and monoclonal antibodies for cancer treatment. The key difference between conventional biologicals and CTGTPs is that while proteins are the final products in conventional biologicals, cells are the final products in CTGTPs. Cells can produce specific proteins continuously as compared to the fixed number of specific proteins, which may be degraded and thus depleted in the body. Hence, the cells can potentially allow for longer lasting or permanent prophylaxis. In general, the manufacturing process for chimeric antigen receptor T (CAR-T) cell therapy products, one of the most common CTGTPs, involves steps to preserve the cells and focus on purifying specific target cells, while biologicals manufacturing involves an additional step of isolation and purification of the protein. Since cells are relatively more sensitive to their environment, a more stringent process in terms of the manufacturing environment must be in place to maintain the quality and safety of the CTGTP. Overall, cell therapy products are generally not as well characterized as compared to conventional biologicals, thus having different biomarkers in testing for efficacy.
Table 1 shows examples of the different types of products and how they work. Figure 1 focuses on the manufacturing process of CAR-T cell therapy product and conventional biologicals. Table 2 gives further details regarding the manufacturing, quality control storage and transport between CTGTPs and conventional biologicals.
Official definitions of CTGTPs
In general, most countries adopt a risk-based approach in deciding if a product is a CTGTP before subjecting it to licensing requirements. In countries such as the United States (US), the European Union (EU), and South Korea, minimally manipulated and homologous use products are not subject to marketing authorization. For CTGTPs which require marketing authorisation, the extent of regulatory requirements depends on the type of products manufactured. Countries such as Singapore include minimally manipulated and homologous products under its definition of CTGTPs, and specifically exclude other products of the same type, e.g. bone marrow, peripheral blood, cord blood and vaccines, without further classifying them as CTGTPs. Other countries such as China and India have no formal definitions for CTGTPs.
Table 3 states the definitions and classifications by the US, EU, Australia, Japan, China, India, Malaysia, Thailand, Singapore, South Korea, the World Health Organization (WHO) and the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). These countries have been chosen to represent a heterogeneous regulatory environment with differing levels of capacity and maturity.
Manufacturing of CTGTPs
In the manufacture and commercialization of CTGTP, two main modes of manufacturing styles exist. Decentralized manufacturing spreads production over different locations, allowing for a more amenable response to demands [41]. An example of a decentralized manufacturing process is the integration of good manufacturing practice (GMP) facilities into a hospital setting to produce autologous therapies for patients. However, certain risks are associated with this model, including difficulty in quality control due to a lack of central oversight and contamination risk [42]. On the other hand, centralized manufacturing has been the prevalent way of manufacturing as it enables an economy of scale, due to well-established processes and machinery to produce large, standardized batches of the same product at a single location [41]. Some examples include chemical drugs, allogeneic products and biologicals. However, this characteristic makes it difficult for manufacturers to customize products for specific patients. Currently, centralized manufacturing is utilized for licensed CTGTPs such as Kymriah (Novartis) and Yescarta (Gilead), with a substantial interest in moving towards decentralized manufacturing for autologous products at the point of care [8]. The advantages and disadvantages of the manufacturing methods will be further discussed in the subsequent sections.
As mentioned, the unique nature of CTGTPs as compared to conventional biologicals makes the manufacturing of safe and efficacious CTGTPs a challenge. So far, there has been a clear distinction between manufacturing for product development and conducting clinical trials for academic research, with the former taking place in pharmaceutical companies and the latter in hospitals. However, in recent developments, personalized CTGTPs have demanded a higher involvement of hospitals in the development of CTGTPs due to their manufacturing process [20], which must be near to the patient due to the sensitivity of the product, thus necessitating hospital premises to be of GMP standard. The problems of quality control in cell therapies produced in the academic setting and industry, coupled with strict regulations and difficulty in harmonizing a standardized manufacturing process, hinder the availability of treatments to patients [43] through manufacturing process challenges.
The manufacturing process of CAR-T cells is shown in Figure 2. Peripheral blood mononuclear cells are first collected from the patient via leukapheresis. This is followed by T-cell selection, removing adulterants such as gross red blood cells and platelets, while simultaneously enriching T cells [18]. The T cells are then activated using technologies involving antibody-coated nanobeads before being transduced with a viral vector, which contains the anti-CD19 CAR transgene. The T cells are then expanded in bioreactors to produce doses for sufficient therapeutic effect. Finally, the T cells are removed from the beads, washed, cryopreserved in infusion bags, and tested for the critical quality attributes of the product before it is released and thawed for infusion into the patient [44].
In the case of tissue engineering and regenerative medicine (TERM) therapies, multiple types of materials are required to come together. As such, the manufacturing workflow is different for each component, including cells, scaffolds or bio-printed therapies. The manufacturing workflow for cells is as shown in Figure 2, whilst the manufacturing workflow for scaffolds and bio-printed materials are shown in Figure 3. Bioprinting involves the fabrication of three-dimensional anatomical structures to be used in therapies [45] and in in vitro models since they can be engineered to mimic physiological tissues to a high degree [6]. Other components may include signalling molecules or medical devices [45].
Premises and equipment
Since CTGTPs cannot be terminally sterilized, they must be aseptically processed as stipulated under national and international CTGTP guidelines, including those of Singapore HSA. This means that a Grade A environment with a Grade B background for open systems, or a Grade D background for closed systems, including isolators, are used to reduce the number of contaminants in an aseptic environment [1]. The relevant cleanroom requirements are listed in Table 4, together with an example of a cleanroom in Figure 4. To reduce the risk of contamination, a closed system is typically preferred, as an open processing system allows for materials to be exposed to the room’s environment. A closed processing system consists of closed tubing pathways and connections, incorporating pre-sterilized, single-use components [46], thus eliminating the introduction of adventitious agents. This allows for flexibility and space in process design for regulatory compliance since materials of closed systems are pre-assembled [47], with closed, automated systems such as the CliniMACS Prodigy from Miltenyi which can perform cell preparation, enrichment, activation, transduction, expansion and purification, allowing for easy integration into manufacturing strategies [48]. A Grade D cleanroom environment also equates to less strict ventilation, cleaning, and gowning requirements [20] which can reduce financial costs. However, due to the novelty of closed process technology, many personnel are still unfamiliar with using the technology, thus preferring the traditional process of biomanufacturing [47]. Additionally, the healthcare technology that is available at hospitals is often not enough to meet all GMP requirements, such as installation, operation and maintenance which require suitably qualified technicians to implement them, often leading to the outsourcing of these activities [48]. Currently, a small number of cell-processing facilities in CTGTP manufacturing are closed systems; however, they are anticipated to increase in the years to come [49].
Materials and processing
Starting material Since the initial cell populations are obtained from the patients themselves in autologous cell therapies, they can be highly heterogeneous as the quality of the cells depends on the patient’s health. This can reduce the reproducibility and definition of the final product [24]. With a limited amount of starting material available from the patient, the amount of material available for quality control test methods may be correspondingly limited. Thus, the sampling strategies to ensure a sufficient final product dose for patients may in turn affect the accuracy of the test results which reflects the properties of a batch of CTGTP [48]. Several cell types are also adherent in nature, requiring detachment from cultures in their intact form before being processed downstream, thus potentially affecting cell quality [3]. Furthermore, cells are highly sensitive to their environment and display changing behaviours in response, further contributing to their variability [51]. Patients receiving the therapy are also cancer patients who undergo aggressive therapies which can affect T-cell fitness negatively, leading to failure in product generation altogether [52].
Next, as the biophysical properties of full and empty viral capsids are similar, it is a challenge to separate them. This can result in them being processed together, causing the final product to contain both kinds of vectors during the delivery of genetic materials into the cells. If many empty vectors are present, a larger therapeutic dose may be needed, which may lead to adverse immune reactions in patients [53].
For tissue-engineered products, additional materials such as cells, scaffolds and signalling molecules are required to be combined during the manufacture of the product, thus increasing the complexity of the manufacturing process. In addition, there is much uncertainty in terms of whether signalling molecules can bring about the desired cellular differentiation, whether the scaffold supports cellular growth and vascularisation or whether the product has the desired structural properties [7].
Quality control Due to the limited amount and variability of the material, the traditional approach of process validation can be difficult to perform, especially for autologous products, as it requires multiple successful production batches to be evaluated and potential changes to be made to critical processes, equipment and materials subsequently. Additionally, as the mechanism of actions for cells are not well recognized, the critical quality attributes (CQAs) associated with measurable product attributes for assuring functional quality and reproducibility cannot be determined [54].
The intrinsic variability of cells also contributes to the variability of critical process parameters (CPPs). In the use of cells in tissue engineering, purity is assured since characterization has been achieved for differentiated cells. However, pluripotent cells would require 100% purity to avoid tumorigenicity, thus creating ambiguity in the assessment of their safety and efficacy [55]. Each component, such as the production of scaffolds, would require the maintenance of their quality attributes before seeding them with cells, raising the complexity of tissue-engineered products [45].
The monitoring of CPPs, such as culture conditions, which are elements of the production process that affect CQAs such as cell quality and reproducibility across multiple batches and manufacturing sites have not been established. Extensive data analytics and models would thus have to be used to identify sets of markers (as CQAs) from animal studies and clinical trials to establish product safety [54]. Currently, there is a shortage of robust process analytical technologies (PATs) to examine CPPs for cell-expansion and other processes. Although PAT devices that monitor pH, dissolved oxygen (DO), and other biopharmaceutical CPPs have improved significantly in terms of miniaturization and integration, the manufacture and quality control of CTGTPs are still using monitoring or detection devices that can damage the sample [56]. Overall, CTGTP manufacturing does not currently incorporate quality-by-design principles that allow for high quality and extensive production of therapeutic cells [54].
Cryopreservation Cell function starts to deteriorate after the collection of the sample and continues up to cryopreservation [25]. In cryopreservation, cells are commonly stored in liquid nitrogen at −196◦C. To recover cryopreserved cells, slow freezing and fast thawing are usually performed [57]. The construction of a cryo-chain for extended storage and delivery is pertinent to preventing the decrease in metabolic activity and cell viability as cells go through different stages in the manufacturing process, which may take up to more than 4 weeks due to quality assessments, release controls and shipment in the case of a centralized process [58]. In contrast, a decentralized process takes up to only 2 weeks as there is no need for cryopreservation nor the shipment of T cells, which protects the cells from injury during freezing and thawing [59]. A shortened duration between leukapheresis and infusion also reduces the need for the patient to receive bridging chemotherapy, which is important in controlling disease progression and averting infections from low blood cell count [58]. A patient would need to receive bridging therapy to control disease progression and prevent potential infections due to low blood cell count while waiting for the infusion [58], thus a shortened duration between leukapheresis and infusion in decentralized processes would also cut down on costs of chemotherapy and extended hospital stay [59].
Human resource and accreditation Due to the novelty of technology involved in the manufacturing process, human resources would have to be trained, requiring expertise from biology, engineering and computer science [54]. A survey conducted has shown that human resources in multiple fields such as business expansion and product development, together with researchers possessing a comprehensive scope of qualifications, were much sought after. Personnel with GMP manufacturing experiences were also needed by a large portion of respondents [60]. In the context of centralized processing, the efficient allocation of manpower and equipment can be realized [27], if professionals have a thorough understanding of cryopreservation protocols [25], treatment guidelines and possible complications of CTGTP administration, such as cytokine release syndrome and neurotoxicity [8]. Additionally, physicians tend to be clinically conservative and are unwilling to utilize novel treatments especially if they require atypical methods of delivery, thus necessitating evidence in safety assurance and the ability for processes to integrate into existing clinical practice [61, 62].
Potential solutions to the challenges encountered in manufacturing
Outsourcing Due to the substantial cost of manufacturing CTGTPs, it is important to decide which manufacturing strategy is suitable to cater to a specific product and to design a strong supply chain that can withstand disruptions, such as in a global pandemic where a shortage of materials can result in delayed shipments of cell therapies [63]. One strategy where pharmaceutical start-ups and small developers who lack the resources to manage in-house manufacturing may choose to outsource to contract development and manufacturing companies (CDMO), which are larger and better able to utilize economies of scale [64]. In the absence of trained personnel, it may be prudent to outsource aseptic procedures to avoid potential sterility and contamination issues. If companies struggle to meet guidance standards, they should be strongly encouraged to increase the extent of outsourcing to help in the compliance of GMP standards. It is of critical importance that the CTGTP manufacturing setup complies with GMP standards.
Qualifications Current GMP guidelines for CTGTPs only require healthcare professionals to have appropriate training in terms of aseptic handling and gowning with no specific qualifications or minimum years of training [1]. While these guidelines cannot be too specific due to the wide range of CTGTPs, higher standards are expected for products that have undergone substantial manipulation as opposed to minimally manipulated products, which are allowed to comply with less stringent standards. Going forward it is recommended that a minimum length of relevant working experience be stipulated for personnel handling CTGTPs. It should also be made mandatory for personnel who are directly engaged in CTGTP processing to undergo training and be certified in basic aseptic techniques. Professionals may also be encouraged to participate in further education programmes to increase their scientific knowledge of CTGTPs. This is particularly important as a lack of skills and knowledge can impact the quality of the product significantly. This can be seen from the trends in biologicals manufacturing where mishandling in production and administration has led to substandard and unsafe protein products [65]. As more products undergo clinical trials, more scientific knowledge will be generated, some of which can then be incorporated into regulations. The requirements for personnel qualifications and training may then be more clearly stipulated based on the types of CTGTP products manufactured.
Technology A changing mindset is also necessary in terms of embracing emerging trends of Industry 4.0, including disruptive technologies to improve the comparability of products and to reduce contamination. Technologies can be used to model available data in the calculation of operational feasibility and cost implications to avoid unnecessary cost, as shown in a study by Lam C et al. [66], and to improve the quality of products through robust and non-destructive monitoring techniques.
Control of CTGTPs
Current regulatory framework Table 5 summarizes the regulatory frameworks governing CTGTPs across several jurisdictions. Some are more comprehensive than others in providing for the different types of pathways. Many countries have expedited pathways to cater to the need for CTGTPs to reach patients quickly.
Gaps identified in regulatory control and potential solutions
Risk-based approach The risk-based approach is contingent upon identifying risks associated with the use of a CTGTP in the clinical setting and its inherent risks concerning quality, safety and efficacy. This process starts at the beginning of product development and matures over time, as the knowledge of the product and its characteristics increases [31]. Expedited pathways shorten this process, allowing therapies to reach patients quickly and increase options available, which is important especially in life-threatening diseases. However, this means that less evidence of safety and efficacy is collected, which may impact product quality [74].
Furthermore, manufacturers have no incentive to perform post-marketing promptly due to potential adverse effects leading to drug withdrawal and subsequently a loss of profit. The post-marketing requirements issued by regulators are also scant on details [72, 77]. Robust post-market evidence is essential in facilitating the successful implementation of accelerated approval programmes for the verification of the safety and efficacy of CTGTPs. However, post-market studies largely utilize methods similar to pre-market trials with minimal patient numbers and brief follow-up periods rather than using real-world scenarios for approved ATMPs in the EU [72, 78]. As such, regulations need to achieve the balance between flexibility in accommodating new knowledge and at the same time specific in terms of setting out requirements in data submission.
In terms of GMP standards, the characteristics of CTGTPs should be considered, such as smaller batch sizes and shorter half-lives. As such, it is important to establish GMP standards different from conventional drugs and biologicals that account for the inherent variability of CTGTPs, where out-of-specification (OOS) products may be anticipated. An example would be the approved CAR-T cell therapy product Kymriah (Novartis), where 10% of products could not be shipped due to OOS issues or manufacturing failures. However, OOS Kymriah is still effective with no evidence of higher safety risk as supported by real-world data [79]. Currently, some countries such as Japan and China have already started to move towards incorporating real-world data into submission requirements, evident from China’s ‘Guideline for the use of Real-World Evidence for Research and Regulatory Review’.
International harmonization of definition and scope of policies A key discussion in the enactment of Japan’s Act on the Safety of Regenerative Medicine (ASRM) highlighted the importance of shaping the scope of the regulation and deciding what it would regulate, as it could potentially exclude regulation of important developing therapies [80]. The ASRM has also adopted the term ‘regenerative medicine et cetera’, with ‘et cetera’ providing the flexibility to include technologies not yet discovered and unapproved therapies [80]. Discrepancies in regulatory terminologies such as the definition of CTGTPs led to the approval of the same product under different definitions. For example, tisagenlecleucel was approved as a cell therapy product in Australia and Japan yet approved as a gene therapy product in the US and EU [72]. The criteria for eligibility and application procedures for expedited programmes varied across different countries, where no single product was granted expedited approval under the expedited programmes in the US, EU and Japan [72]. This could discourage manufacturers from seeking approval in foreign countries as they would need to spend additional resources to manoeuvre different regulations, thus limiting patients’ access to therapies.
In line with the harmonization of regulations, there is also a need for greater communication between stakeholders. A study showed that only slightly more than half of companies in Malaysia understood the variances in registration requirements between different product classes [83]. Using the example of Kymriah, the US FDA required the product to consist of minimally 80% viable T cells, different from the 70% which was set during clinical trials. However, real-world data revealed that patients receiving doses of viability below 80% also achieved complete response [79]. Thus, there is a need for more extensive communication between different stakeholders, and flexibility in adjusting parameter ranges when more data is received even after the product has been put out to the market.
Furthermore, no global unified regulatory standards are available as a reference or guidance, especially for countries where the technical reviewers lack experience. Also, there are countries which still do not have specific legislation for CTGTPs, including the lack of ethical laws and human rights protection, or having separate regulatory authorities for clinical trial application and marketing authorization [71] unlike the US or UK.
As such, there is a need for the convergence of international regulations. Social science research has shown that emerging markets are stabilized when consumer confidence is boosted through creating standardized regulations [81, 82]. Currently, international harmonization initiatives, including the Gene and Cell Therapy Working Group of the International Pharmaceutical Regulators Form (IPRF) and ICH, are taking place, with the ICH being the primary organization in generating shared technical guidelines to be utilized by different countries in the harmonization process. However, this requires a long time, which may not be rapid enough in dealing with the speed of innovation in the CTGTP area. As such, convergence may be a more desirable option, where regulatory requirements align across countries by utilizing internationally recognized guidance documents [73]. This also provides time for manufacturers to understand any changes to regulations and to adapt manufacturing processes accordingly. By fostering close international cooperation, less advanced countries can also learn from more advanced countries without the need to abruptly adopt regulation standards, since they may not have the capacity to do so currently without being penalized unnecessarily.
Conclusion
CTGTPs are novel therapy products that seek to address unmet medical needs using materials such as stem cells for a regenerative effect, or through genetic engineering to improve the ability of cells to target cancer cells. Types of therapies include autologous therapies, where the starting material is derived from the patient, and allogeneic therapies, where the starting material is obtained from healthy donors. CTGTPs also differ from conventional biologicals in manufacturing process due to their specific characteristics, such as the need to preserve the quality of the entire cell as compared to conventional biologicals, where the focus is on the quality of the therapeutic protein product. Storage, transport and cryopreservation of CTGTPs in the manufacturing cycle are also important since cells require more extreme cryopreservation temperatures, and additional heterogeneity has to be managed if the therapy product is autologous. As a result, a more stringent process is required in the manufacturing of CTGTPs. Some solutions to the challenges encountered in manufacturing include ensuring appropriate accreditation of professionals handling CTGTPs, using automation and outsourcing to CDMOs to ensure better compliance to GMP standards.
In CTGTP regulation, jurisdictions have defined and categorized CTGTPs largely according to the extent of manipulation and whether it is for homologous use or not, where a larger extent of manipulation requires more stringent regulations. Considering the lack of data from clinical trials due to small clinical trial groups and disease severity, many jurisdictions have put in place expedited pathways to allow products to reach patients faster. In addition, regulations need to be flexible to accommodate new scientific knowledge as the CTGTP field advances. The different levels of regulation across countries serve as a barrier to manufacturers seeking to export CTGTPs overseas. In addition, certain countries also do not have specific legislation in place for CTGTPs such as ethical laws and human rights protection. As such, there is a need for the convergence of international regulations to serve as guidance in drafting new laws and to provide clarity to manufacturers. Many guidance documents are already available, such as the ‘PIC/S Annex 2A for Advanced Therapy Medicinal Products’ to guide manufacturers, as new scientific knowledge continues to emerge and evolve. With the help of international organizations, the harmonization of regulations across the world is slowly beginning to materialize, providing guidance and greater clarity to countries that lag on regulations. International harmonization can also minimize the duplication of clinical trials and streamline the process of granting marketing authorizations for CTGTPs, thereby fostering innovation. There should also be greater and more effective communication between the regulator and different stakeholders such as manufacturers, with feedback and some degree of flexibility incorporated into regulations.
The COVID-19 pandemic has accelerated digital transformation and exposed weak areas in pharmaceutical supply chains. At the same time, this has also presented opportunities for manufacturers and regulators to utilize technology to tackle the challenges of CTGTP manufacturing through new and innovative ways, ultimately improving the accessibility of these ground-breaking medicines to patients.
Competing interests: None.
Provenance and peer review: Not commissioned; externally peer reviewed.
Authors
Adjunct Associate Professor Sia Chong Hock, BSc (Pharm), MSc
Christine Koh, BSc (Pharm) (Hons) Associate Professor Chan Lai Wah, BSc (Pharm) (Hons), PhD
Department of Pharmacy, National University of Singapore, 18 Science Drive 4, Singapore 117543
References 1. Health Sciences Authority. Guidance documents for CTGTP [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.hsa.gov.sg/ctgtp/guidance-documents 2. Tretiakova AP. Realizing the promise of gene therapy through collaboration and partnering: Pfizer’s view [homepage on the Internet]. Scientific American. 2019 Jan 14. 3. Heathman TR, Nienow AW, McCall MJ, Coopman K, Kara B, Hewitt CJ. The translation of cell-based therapies: clinical landscape and manufacturing challenges. Regen Med. 2015;10(1):49-64. 4. Goswami R, Subramanian G, Silayeva L, Newkirk I, Doctor D, Chawla K, et al. Gene therapy leaves a vicious cycle. Front Oncol. 2019;9:297. 5. Belete TM. The current status of gene therapy for the treatment of cancer. BTT. 2021;15:67-77. 6. Chandra PK, Soker S, Atala A. Tissue engineering: current status and future perspectives. In: Principles of Tissue Engineering. Elsevier; 2020. p. 1-35. 7. Gerlovin L, Thompson A, Vailas J. Untapped potential tissue engineering: the three obstacles holding it back. BioProcess Intl. 2021 Apr 26. 8. RESTORE – large scale research initiative in Europe [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.restore-horizon.eu/ 9. Association for the Advancement of Blood & Biotherapies. Facts about cellular therapies [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.aabb.org/news-resources/resources/cellular-therapies/facts-about-cellular-therapies 10. World Health Organization. Guidelines on the quality, safety and efficacy of biotherapeutic protein products prepared by recombinant DNA technology, Annex 4, TRS No 987. 18 June 2014 [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.who.int/publications/m/item/recombinant-dna-annex-4-trs-no-987 11. European Medicines Agency. Spherox. 2018 [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/spherox 12. Stein AM, Grupp SA, Levine JE, Laetsch TW, Pulsipher MA, Boyer MW, et al. Tisagenlecleucel model‐based cellular kinetic analysis of chimeric antigen receptor–t cells. CPT Pharmacometrics Syst Pharmacol. 2019;8(5):285-95. 13. Novartis. The science of car-T cell therapy [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.novartis.com/our-focus/cell-and- gene-therapy/car-t/car-t-healthcare-professionals/science-car-t-cell-therapy 14. Cure SMA. Zolgensma [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.curesma.org/zolgensma/ 15. About VergenixTM FG [homepage on the Internet]. [cited 2022 Mar 11]. Available from: http://vergenixfg.com/about/ 16. Farid SS, Jenkins MJ. Bioprocesses for cell therapies. In: Biopharmaceutical Processing. Elsevier; 2018. p. 899-930. 17. Apte A, Afuwape A, Buljovcic Z, Younes Z. Manufacture and regulation of cell, gene and tissue therapies, Part 1: chemistry, manufacturing, and control challenges. BioProcess Int. 2020. 18. Wang X, Rivière I. Clinical manufacturing of CAR T cells: foundation of a promising therapy. Mol Ther Oncolytics. 2016;3:16015. 19. Sia CH, Sia MK, Chan LW. Global challenges in the manufacture, regulation and international harmonization of GMP and quality standards for biopharmaceuticals. Generics and Biosimilars Initiative Journal (GaBI Journal). 2020;9(2):52-63. doi:10.5639/gabij.2020.0902.010 20. Iancu EM, Kandalaft LE. Challenges and advantages of cell therapy manufacturing under Good Manufacturing Practices within the hospital setting. Curr Opin Biotechnol. 2020;65:233-41. 21. Sterling J. Scaling up cell therapy manufacturing. Genet Eng Biotechnol News. 2018 Sep 7. 22. Morenweiser R. Downstream processing of viral vectors and vaccines. Gene Ther. 2005;12(Suppl 1):S103-10. 23. Murray C, Pao E, Jann A, Park DE, Di Carlo D. Continuous and quantitative purification of T-cell subsets for cell therapy manufacturing using magnetic ratcheting cytometry. SLAS Technol. 2018;23(4):326-37. 24. Roh K-H, Nerem RM, Roy K. Biomanufacturing of therapeutic cells: state of the art, current challenges, and future perspectives. Annu Rev Chem Biomol Eng. 2016;7(1):455-78. 25. Meneghel J, Kilbride P, Morris GJ. Cryopreservation as a key element in the successful delivery of cell-based therapies—a review. Front Med (Lausanne). 2020;7:592242. 26. Schuck RN, Grillo JA. Pharmacogenomic biomarkers: an FDA perspective on utilization in biological product labeling. AAPS J. 2016;18(3):573-7. 27. Quintarelli C, Locatelli F, Caruana I, De Angelis B. Overcoming challenges in car t-cell product CGMP release. Mole Ther. 2016;24(5):845-6. 28. Abou-El-Enein M, Elsanhoury A, Reinke P. Overcoming challenges facing advanced therapies in the EU market. Cell Stem Cell. 2016;19(3):293-7. 29. Mirasol F. New therapies present scaling challenges. BioPharm. 5 Dec 2019. 30. U. S. Food and Drug Administration [homepage on the Internet]. 2021 [cited 2022 Mar 11]. Available from: https://www.fda.gov/home 31. European Medicines Agency [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.ema.europa.eu/en. 32. Pharmaceutical Inspection Co-operation Scheme [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://picscheme.org/ 33. Pharmaceuticals and Medical Devices Agency. [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.pmda.go.jp/ 34. National Medical Products Administration. Notice of the General Administration on issuing the technical guidelines for the research and evaluation of cell therapy products (2017 No. 216) [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.nmpa.gov.cn/ylqx/ylqxggtg/ylqxzhdyz/20171222145101557.html 35. Government of India. Department of Biotechnology, Ministry of Science & Technology. Stem cells regenerative medicine [cited 2022 Mar 11]. Available from: https://dbtindia.gov.in/schemes-programmes/research-development/medical-biotechnology/stem-cells-regenerative-medicine 36. Australian Government. Department of Health. Therapeutic Goods Administration. Classification of biologicals [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.tga.gov.au/classification-biologicals 37. Jaringan Dokumentasi dan Informasi Hukum Badan Pengawas Obat dan Makanan RI [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://jdih.pom.go.id/ 38. FDA Thailand [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.fda.moph.go.th/sites/fda_en/Pages/Main.aspx 39. Korean Legislation Research Institute [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://elaw.klri.re.kr/ 40. World Health Organization [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.who.int. 41. Harrison RP, Ruck S, Rafiq QA, Medcalf N. Decentralised manufacturing of cell and gene therapy products: learning from other healthcare sectors. Biotechnol Adv. 2018;36(2):345-57. 42. Medcalf N. Business models for manufacture of cellular therapies. In: Stem cell manufacturing. Elsevier; 2016. p. 265-90. 43. Egri N, Ortiz de Landazuri I, San Bartolomé C, Ortega JR, Español-Rego M, Juan M. CART manufacturing process and reasons for academy-pharma collaboration. Immunol Lett. 2020;217:39-48. 44. Tyagarajan S, Spencer T, Smith J. Optimizing CAR-T cell manufacturing processes during pivotal clinical trials. Mol Ther Methods Clin Dev. 2020;16:136-44. 45. Hunsberger J, Harrysson O, Shirwaiker R, Starly B, Wysk R, Cohen P, et al. Manufacturing road map for tissue engineering and regenerative medicine technologies: manufacturing road map for term. Stem Cells Transl Med. 2015;4(2):130-5. 46. Hampson B. Closed processing for cell therapies. Genet Eng Biotechnol News. 2014;34(9). 47. Paul Mueller Company Academy. Open vs closed bioprocessing [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://academy.paulmueller.com/open-vs.-closed-bioprocessing 48. Viganò M, Giordano R, Lazzari L. Challenges of running a GMP facility for regenerative medicine in a public hospital. Regen Med. 2017;12(7):803-13. 49. Bream A, Salzmann B. The difficulties of manufacturing cell and gene therapies at scale. BioProcess Intl. 2021. 50. Evren A, Pontus B. GMP facilities for manufacturing of advanced therapy medicinal products for clinical trials: an overview for clinical researchers. Curr Gene Ther. 2010;10(6):508-15. 51. Garcia-Aponte OF, Herwig C, Kozma B. Lymphocyte expansion in bioreactors: upgrading adoptive cell therapy. J Biol Eng. 2021;15(1):13. 52. Caldwell KJ, Gottschalk S, Talleur AC. Allogeneic CAR cell therapy—more than a pipe dream. Front Immunol. 2021;11:618427. 53. Mirasol F. Challenges in vector purification for gene therapy. BioPharm Int. 2020;33(2):22-3. 54. Dwarshuis NJ, Parratt K, Santiago-Miranda A, Roy K. Cells as advanced therapeutics: state-of-the-art, challenges, and opportunities in large scale biomanufacturing of high-quality cells for adoptive immunotherapies. Adv Drug Deliv Rev. 2017;114:222-39. 55. Gardner J, Webster A. The social management of biomedical novelty: facilitating translation in regenerative medicine. Soc Sci Med. 2016;156:90-7. 56. Bure K, Lipsitz Y, Lowdell M, Wall I, Zandstra P. Quality by design for advanced therapies: an informed route to enhanced late-stafe clinical success and empowered process flexibility. BioProcess Int. 2020. 57. Nath SC, Harper L, Rancourt DE. Cell-based therapy manufacturing in stirred suspension bioreactor: thoughts for cGMP compliance. Front Bioeng Biotechnol. 2020;8:599674. 58. Buechner J, Kersten MJ, Fuchs M, Salmon F, Jäger U. Chimeric antigen receptor-T cell therapy: practical considerations for implementation in Europe. Hemasphere. 2018;2(1):e18. 59. Ran T, Eichmüller SB, Schmidt P, Schlander M. Cost of decentralized CAR T ‐ cell production in an academic nonprofit setting. Int J Cancer. 2020;147(12):3438-45. 60. Nishigaki F, Ezoe S, Kitajima H, Hata K. Human resource development contributes to the creation of outstanding regenerative medicine products. Regen Ther. 2017;7:17-23. 61. O’Donnell BT, Ives CJ, Mohiuddin OA, Bunnell BA. Beyond the present constraints that prevent a wide spread of tissue engineering and regenerative medicine approaches. Front Bioeng Biotechnol. 2019;7:95. 62. Dlaska CE, Andersson G, Brittberg M, Suedkamp NP, Raschke MJ, Schuetz MA. Clinical translation in tissue engineering—the surgeon’s view. Curr Mol Bio Rep. 2015;1(2):61-70. 63. Qiu T, Wang Y, Liang S, Han R, Toumi M. The impact of COVID-19 on the cell and gene therapies industry: disruptions, opportunities, and future prospects. Drug Discov Today. 2021;26(10):2269-81. 64. Michael L. Manufacturing cures: infrastructure challenges facing cell and gene therapy developers. Pharma Intelligence. In vivo. 2019. 65. Vulto AG, Jaquez OA. The process defines the product: what really matters in biosimilar design and production? Rheumatology (Oxford). 2017;56(Suppl 4):iv14-iv29. 66. Lam C, Meinert E, Yang A, Cui Z. Comparison between centralized and decentralized supply chains of autologous chimeric antigen receptor T-cell therapies: a UK case study based on discrete event simulation. Cytotherapy. 2021;23(5):433-51. 67. Mendicino M, Fan Y, Griffin D, Gunter KC, Nichols K. Current state of U.S. Food and Drug Administration regulation for cellular and gene therapy products: potential cures on the horizon. Cytotherapy. 2019;21(7):699-724. 68. Detela G, Lodge A. EU regulatory pathways for ATMPs: standard, accelerated and adaptive pathways to marketing authorisation. Mol Ther Methods Clin Dev. 2019;13:205-32. 69. Bishop S, Flight S, Thomas N. The regulatory environment for cell therapies in Australia – an opportunity to expedite clinical development. Cell Geni Ther Insights. 2018;4(6):523-33. 70. Australian Government. Department of Health. Therapeutic Goods Administration. Australian regulatory guidelines for biologicals (ARGB) [homepage on the Internet]. 2021 [cited 2022 Mar 11]. Available from: https://www.tga.gov.au/publication/australian-regulatory-guidelines-biologicals-argb 71. Parexel Academy [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://parexel-academy.com 72. Qiu T, Hanna E, Dabbous M, Borislav B, Toumi M. Regenerative medicine regulatory policies: a systematic review and international comparison. Health Policy. 2020;124(7):701-13. 73. Drago D, Foss-Campbell B, Wonnacott K, Barrett D, Ndu A. Global regulatory progress in delivering on the promise of gene therapies for unmet medical needs. Mol Ther Methods Clin Devel. 2021;21:524-9. 74. DIA [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.diaglobal.org/en 75. Korea Biomedicine Industry Association [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://www.kobia.kr/bbs/board.php?tbl=e_newsletter&mode=VIEW&num=72& 76. The International Council for Harmonisation [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://ich.org/ 77. Hoekman J, Klamer TT, Mantel‐Teeuwisse AK, Leufkens HGM, De Bruin ML. Characteristics and follow‐up of postmarketing studies of conditionally authorized medicines in the EU. Br J Clin Pharmacol. 2016;82(1):213-26. 78. Fritsche E, Elsallab M, Schaden M, Hey SP, Abou-El-Enein M. Post-marketing safety and efficacy surveillance of cell and gene therapies in the EU: a critical review. Cell & Gene Therapy Insights. 2019;5(11):1505-21. 79. Novartis still hasn’t solved its CAR-T manufacturing issues [homepage on the Internet]. BioPharma Dive. 11 Dec 2019. 80. Takashima K, Morrison M, Minari J. Reflection on the enactment and impact of safety laws for regenerative medicine in Japan. Stem Cell Reports. 2021;16(6):1425-34. 81. Tiwari SS, Raman S, Martin P. Regenerative medicine in India: trends and challenges in innovation and regulation. Regen Med. 2017;12(7):875-85. 82. Charles Edquist [homepage on the Internet]. [cited 2022 Mar 11]. Available from: https://charlesedquist.com/ 83. Loh EYX, Goh PS, Mannan AMM, Mohd Sani N, Ab Ghani A. Cell and gene therapy products in Malaysia: a snapshot of the industry’s current regulation preparedness. Cytotherapy. 2021;23(12):1108-13.
Author for correspondence: Adjunct Associate Professor Sia Chong Hock, BSc (Pharm), MSc, Department of Pharmacy, National University of Singapore, 18 Science Drive 4, Singapore 117543
Disclosure of Conflict of Interest Statement is available upon request.
Permission granted to reproduce for personal and non-commercial use only. All other reproduction, copy or reprinting of all or part of any ‘Content’ found on this website is strictly prohibited without the prior consent of the publisher. Contact the publisher to obtain permission before redistributing.
GaBI Journal is an independent and peer reviewed academic journal. GaBI Journal encompasses all aspects of generic and biosimilar medicines development and use, from fundamental research up to clinical application and policies.